https://dx.doi.org/10.24016/2026.v12.487
ORIGINAL ARTICLE
Factor structure of the Work-Related Acceptance and Action Questionnaire
in health personnel
Jesus Blancas-Guillen 1 *, Leandra Ccoyllo-Gonzalez
1, Giuliana Salazar-Alvarez 2,3, Franco
Andree Méndez-Flores 4, Pablo D. Valencia 5
1 Instituto Peruano de Psicología Contextual – Dirección
Valiosa, Lima, Peru.
2 Asociación Peruana Contextual-Conductual de Psicología,
Lima, Peru.
3 Universidad Peruana Cayetano Heredia, Lima, Peru.
4 Departamento de Psicología, Universidad Iberoamericana, Mexico
City, Mexico.
5 Coordinación de Universidad Abierta y Educación Digital,
Universidad Nacional Autónoma de México, Mexico City, Mexico.
* Correspondence: blancasj864@gmail.com
Received: November 17, 2025 | Revised: December 28, 2025 | Accepted: February 10, 2026 | Published Online: March 07, 2026.
CITE IT AS:
Blancas-Guillen, J., Ccoyllo-Gonzalez, L., Salazar-Alvarez,
G., Méndez-Flores, F. A., & Valencia, P. D. (2026). Factor structure of the
Work-Related Acceptance and Action Questionnaire in health personnel. Interacciones, 12,
e487. https://doi.org/10.24016/2026.v12.487
ABSTRACT
Introduction: Acceptance and Commitment Therapy (ACT) has gained
increasing empirical support in workplace settings, highlighting the need for
valid measures of psychological flexibility among healthcare professionals.
Objective: The objective of this study was to examine the
unidimensional structure of the Work-Related Acceptance and Action
Questionnaire (WAAQ), evaluate its internal consistency reliability, and assess
validity evidence based on its associations with anxiety and depression.
Method: The participants were 182 Peruvian healthcare
professionals who completed the WAAQ, the Patient Health Questionnaire-2
(PHQ-2), and the Generalized Anxiety Disorder Scale-2 (GAD-2).
Results: Confirmatory factor analysis supported the one-factor
model (CFI > 0.95, TLI > 0.95, RMSEA < 0.06, and SRMR < 0.08), and
the scale demonstrated adequate internal consistency (ω = 0.87). As
expected, psychological flexibility showed a small-to-moderate correlation with
depression (rs = -0.28, IC 95% [-0.41, -0.14],
p < 0.001) and a moderate correlation with anxiety (rs
= -0.30, IC 95% [-0.42, -0.16], p < 0.001).
Conclusion: The findings suggest that the WAAQ is a valid and
reliable measure of psychological flexibility in the workplace among healthcare
professionals.
Keywords: psychological flexibility, validation study, Acceptance and Commitment
Therapy, healthcare professionals, Peru.
INTRODUCTION
Acceptance and Commitment Therapy (ACT) is considered
part of the third wave of behavioral therapies (Hayes, 2004) and is grounded in
functional contextualism (Biglan & Hayes, 1996).
This perspective views human suffering as inherent to life due to our verbal
nature and emphasizes cognition and language through Relational Frame Theory
(RFT; Hayes et al., 2001). Notably, ACT does not focus on symptom reduction or elimination
but rather on helping individuals accept private events while continuing to
pursue a meaningful life—in other words, fostering psychological flexibility
(Hayes et al., 2014; Wilson & Luciano, 2002). ACT is a transdiagnostic
approach that conceptualizes psychopathology in terms of psychological
inflexibility, where experiential avoidance disorder (EAD) is understood as
part of this inflexible pattern (Hayes et al., 1996; Luciano & Hayes,
2001).
Psychological inflexibility is considered a condition
of psychological vulnerability. Interventions targeting this construct have
been shown to reduce maintaining factors and etiological processes of various
health problems in general and psychological disorders in particular (Kashdan
et al., 2006). These include depression (Bond et al., 2011) and generalized
anxiety disorder (Roemer & Orsillo, 2005). From a transdiagnostic
perspective, psychological inflexibility provides a novel framework for understanding
psychopathology.
The opposite construct, psychological flexibility, was
described by Hayes et al. (2006) as “the capacity to contact the present moment
more fully as a conscious human being and to change or persist in behavior when
doing so serves valued ends” (p. 7). In occupational contexts, greater
psychological flexibility has been linked to improved behavioral effectiveness
at work (Bond et al., 2008), as well as to mental health outcomes (Bond &
Bunce, 2003), job performance (Bond & Flaxman, 2006), and the development
of work-related skills (Hayes et al., 2006). Recent studies with healthcare
professionals have further examined this construct (Bond et al., 2011; Holmberg
et al., 2019; Ortiz-Fune, 2019; Valiente-Barroso et al., 2021). The application
of ACT in healthcare settings has shown promising results, including
improvements in productivity and occupational functioning (Gaupp et al., 2020),
as well as reductions in distress and improvements in mental health (Barrett
& Stewart, 2021; Prudenzi et al., 2021).
To provide a specific measure of psychological
flexibility in occupational settings, Bond et al. (2013) developed the
Work-Related Acceptance and Action Questionnaire (WAAQ). Based on exploratory
factor analyses (EFA), they generated a final version with seven items loading
on a single factor. Confirmatory factor analysis (CFA) subsequently indicated
good fit for the unidimensional model (CFI = .95–.98, RMSEA = .05–.08). The
WAAQ has since been adapted into Spanish (Ruiz & Odriozola-González, 2014),
Chinese (Xu et al., 2018), and Swedish (Holmberg et al., 2019). These studies,
however, used principal components analysis, a method like EFA but not
recommended for analyzing psychological constructs (Lloret-Segura et al.,
2014). More recent studies have also highlighted concerns about the
inappropriate application of EFA and have proposed recommendations to improve
methodological rigor (Paniagua, 2022; Leal-Soto et al., 2022). Given that the
unidimensional structure has been consistently demonstrated, the next logical
step is to test this model directly using CFA (Bond et al., 2013). Furthermore,
although prior research estimated internal consistency using Cronbach’s alpha
(ranging from .81 to .92), current recommendations favor reliability estimates
derived from CFA, such as coefficient omega (Dunn et al., 2014; Savalei & Reise, 2019).
In light of these considerations, it is important to
examine the psychometric properties of the WAAQ using statistical methods
better suited to its nature. Additionally, it is important to assess how this
instrument functions in contexts different from those in which it was initially
developed. The present study therefore pursued three objectives: (a) to
evaluate the unidimensional structure of the WAAQ using CFA; (b) to estimate
internal consistency reliability using coefficient omega; and (c) to examine validity
evidence based on associations with other variables (specifically anxiety and
depression, for which negative correlations were expected). These objectives
were addressed in a sample of healthcare workers in a middle-income country
(Peru) during the COVID-19 pandemic.
METHODS
Design
This was an instrumental study.
Participants
The sample was selected through non-probabilistic
convenience sampling. Inclusion criteria required participants to be formal
Peruvian healthcare workers who understood and accepted the informed consent.
No formal exclusion criteria were established for the study. Before
recruitment, the minimum sample size was determined via a Monte Carlo
simulation using the factor loadings from the Spanish validation of the WAAQ
(Ruiz & Odriozola-González, 2014). Results indicated that a sample size of
150 was sufficient to achieve a statistical power of 1.00 and coverage
probabilities close to 0.95, with negligible parameter and standard error bias
(< 1.5%). Therefore, the final sample consisted of 182 Peruvian healthcare
professionals (55 men and 127 women). Of these, 66.5% were from Metropolitan
Lima and 33.5% from other regions of the country. In terms of employment, 41.2%
worked in the private sector, 37.9% in the public sector, and 20.9% in both
sectors. Psychologists represented the largest professional group (26.9%).
Regarding years of service, 39% had less than 3 years of work experience, while
18.1% had more than 10 years (see Table 1).
|
Table 1. General Characteristics of the Study Sample. |
|||
|
Variable |
|
n |
% |
|
Sex |
Male |
55 |
30.2 |
|
|
Female |
127 |
69.8 |
|
Marital status |
Single |
106 |
58.2 |
|
Married or cohabiting |
65 |
35.7 |
|
|
|
Divorced, separated, or widowed |
11 |
6 |
|
Occupation |
Nurse |
27 |
14.8 |
|
Physiotherapist |
18 |
9.9 |
|
|
Laboratory technician |
8 |
4.4 |
|
|
Physician |
29 |
15.9 |
|
|
Nutritionist |
8 |
4.4 |
|
|
Midwife |
3 |
1.6 |
|
|
Dentist |
15 |
8.2 |
|
|
Psychologist |
49 |
26.9 |
|
|
Pharmacist |
8 |
4.4 |
|
|
Occupational therapist |
2 |
1.1 |
|
|
Speech therapist |
3 |
1.6 |
|
|
Social worker |
2 |
1.1 |
|
|
|
Other |
10 |
5.5 |
|
Work region |
Metropolitan Lima |
121 |
66.5 |
|
|
Rest of the country |
61 |
33.5 |
|
Do you
have children? |
No |
111 |
61 |
|
|
Yes |
71 |
39 |
|
COVID-19 vaccination status |
None |
3 |
1.6 |
|
Two doses |
35 |
19.2 |
|
|
|
Three doses |
144 |
79.1 |
|
Have you had
COVID-19? |
No |
57 |
31.3 |
|
|
Yes |
125 |
68.7 |
|
Work sector |
Public |
69 |
37.9 |
|
Private |
75 |
41.2 |
|
|
|
Both |
38 |
20.9 |
|
Years of service |
< 3 years |
71 |
39 |
|
3 - 5 years |
49 |
26.9 |
|
|
6 - 10 years |
29 |
15.9 |
|
|
|
> 10 years |
33 |
18.1 |
|
Work shift |
Daytime |
106 |
58.2 |
|
Nighttime |
5 |
2.7 |
|
|
|
Rotating |
71 |
39 |
|
Work modality |
On-site |
133 |
73.1 |
|
Remote |
17 |
9.3 |
|
|
|
Hybrid |
32 |
17.6 |
|
Do you take work home? |
No |
116 |
63.7 |
|
|
Yes |
66 |
36.3 |
|
Weekly working hours |
< 40 hours |
83 |
45.6 |
|
41 - 48 hours |
62 |
34.1 |
|
|
49 - 60 hours |
23 |
12.6 |
|
|
|
> 60 hours |
14 |
7.7 |
|
Are you the sole income
provider |
No |
127 |
69.8 |
|
in your household? |
Yes |
55 |
30.2 |
Variables
Work-Related Acceptance and Action Questionnaire (WAAQ; Bond et al., 2013): The WAAQ consists of seven items rated on a
7-point Likert scale ranging from 1 (never true) to 7 (always true), with
higher scores indicating greater work-related psychological flexibility. The
instrument has demonstrated convergent, concurrent, and predictive validity. In
previous studies, internal consistency was acceptable, with Cronbach’s alpha
coefficients of 0.83 and 0.81 in two samples of British workers (Bond et al.,
2013) and 0.92 in a sample of Spanish workers (Ruiz & Odriozola-González,
2014). In the present study, we used the Spanish version validated by Ruiz and
Odriozola-González (2014). This version was reviewed by the Peruvian authors,
who identified no regionalisms or complex wording that could affect the
Peruvian population. Additionally, this version has been used in Colombia and
Ecuador without language-related difficulties (Bravo et al., 2023; Ponce &
Villar, 2022).
Patient Health Questionnaire-2 (PHQ-2; Kroenke et al., 2003): PHQ-2 includes the two core items of the
PHQ-9, one of the most widely used instruments to assess depressive symptoms
(Persons et al., 2018). It assesses experiences over the past two weeks,
specifically: (1) feeling down, depressed, or hopeless, and (2) having little
interest or pleasure in doing things. Items are rated on a 4-point scale
ranging from 0 (not at all) to 3 (nearly every day). In the present sample,
internal consistency was adequate (α = 0.88; categorical ω = 0.80).
Generalized Anxiety Disorder Scale-2 (GAD-2; Kroenke et al., 2007): GAD-2 consists of two items that assess
emotional and cognitive symptoms of generalized anxiety. Items are rated on the
same 4-point scale as the PHQ-2. In this study, internal consistency was
acceptable (α = 0.78; categorical ω = 0.67).
Procedure
Data were collected through an online survey
administered via Google Forms. Collaborations were established with several
healthcare institutions in Lima and other regions of Peru, which distributed
the link through their social networks. Data collection took place between
December 2021 and February 2022. The survey began with an informed consent form
describing the study’s objectives, voluntary participation, and anonymity. The
project was reviewed and approved by the Ethics Committee and the Research Directorate
of the School of Psychology at Universidad Autónoma
del Perú.
Data analysis
First, we computed descriptive statistics at the item
level (mean, standard deviation, skewness, kurtosis, and item–total
correlations). We then conducted confirmatory factor analysis (CFA) using a
robust maximum likelihood estimator (MLR; Yuan & Bentler, 2000). Although
the items use a 7-point Likert scale, we based this decision on methodological
evidence indicating that maximum likelihood estimators perform similarly to
categorical estimators (e.g., WLSMV) when the number of response categories exceeds
five (Rhemtulla et al., 2012). Furthermore, treating
the data as continuous avoids potential instability in estimation associated
with calculating polychoric correlations (e.g., zero
frequencies in contingency tables) in moderate sample sizes.
We evaluated model fit using the Comparative Fit Index
(CFI), the Tucker–Lewis Index (TLI), the Root Mean Square Error of
Approximation (RMSEA), and the Standardized Root Mean Square Residual (SRMR).
We used the following criteria to indicate adequate fit: CFI > 0.95, TLI
> 0.95, RMSEA < 0.06, and SRMR < 0.08. When fit indices were not
satisfactory, we examined modification indices to identify possible respecifications, provided they had theoretical
justification. Based on the CFA results, we estimated internal consistency
reliability using the coefficient omega (ω).
Finally, we examined correlations between WAAQ scores
and anxiety and depression scores. Given the ordinal nature of these variables
and the fact that end users will compute a total observed score by summing the
items, we employed Spearman’s correlations. We conducted all analyses in R
(version 4.0.3) using the lavaan (version 0.6–8) and semTools (version 0.5–3) packages.
Ethical considerations
The Ethics Committee and Research Directorate of the
School of Psychology at the Universidad Autónoma del
Perú approved the protocol. All participants were informed about the study and
provided written informed consent before taking part. The key principles of the
American Psychological Association’s Ethical Principles of Psychologists and
Code of Conduct (2017) were followed. Participation was clearly stated to
be entirely voluntary, and all information collected was handled with the
highest level of confidentiality.
RESULTS
Preliminary Item Analyses
Inspection of
the item statistics indicated that skewness and kurtosis values fell within the
acceptable range of -1 to +1 for most items (except Items 1 and 2). According
to Ferrando and Anguiano-Carrasco (2010), this suggests that the items were
approximately normally distributed. No evidence of floor or ceiling effects was
observed. Item–total correlations exceeded 0.30 for all items (see Table 2).
Table 2. Descriptive Statistics and Item–Total
Correlations for the WAAQ Items.
|
Item |
M |
SD |
g1 |
g2 |
% response per option |
rit |
||||||
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
||||||
|
1 |
5.6 |
1.3 |
-1.2 |
1.6 |
1 |
2.7 |
2 |
13 |
19 |
41 |
22 |
0.7 |
|
2 |
5.6 |
1.2 |
-1.1 |
2 |
1 |
1.6 |
1 |
11 |
25 |
37 |
24 |
0.5 |
|
3 |
5.1 |
1.3 |
-0.8 |
0.7 |
2 |
2.2 |
7 |
17 |
31 |
31 |
11 |
0.8 |
|
4 |
5 |
1.5 |
-0.7 |
0 |
3 |
5.5 |
7 |
17 |
26 |
28 |
2.7 |
0.6 |
|
5 |
5.4 |
1.2 |
-0.8 |
0.8 |
1 |
1.1 |
4 |
16 |
28 |
32 |
18 |
0.7 |
|
6 |
5 |
1.4 |
-0.8 |
0.4 |
3 |
3.3 |
8 |
14 |
30 |
29 |
13 |
0.7 |
|
7 |
5.2 |
1.5 |
-0.9 |
0.5 |
4 |
2.2 |
6 |
18 |
19 |
32 |
20 |
0.6 |
Confirmatory Factor Analysis and Reliability
We conducted a
confirmatory factor analysis to test the proposed dimensionality of the WAAQ
empirically. As shown in Table 3, the one-factor model including all seven
items (Model 1) exhibited poor fit across indices. We proposed a respecified
model allowing the residuals of Items 1 and 3 to correlate (Model 2) due to
their semantic redundancy within the construct of psychological flexibility:
both assess effective work action despite private events (worries vs. nervousness)
and may share method variance due to similar phrasing (e.g., “trabajar eficazmente”). Model 2
demonstrated improved but still suboptimal fit (see Table 3).
Table 3. Fit Indices for the Models Tested Using
Confirmatory Factor Analysis.
|
Model |
χ² |
CFI |
TLI |
RMSEA |
90% CI |
SRMR |
α |
ω |
|
|
LI |
LS |
||||||||
|
Model
1 (gl: 14) |
44.13 |
0.92 |
0.88 |
0.11 |
0.08 |
0.14 |
0.06 |
0.88 |
0.88 |
|
Model
2 (gl: 13) |
27.24 |
0.96 |
0.94 |
0.08 |
0.05 |
0.11 |
0.05 |
0.88 |
0.87 |
|
Model
3 (gl: 9) |
22.08 |
0.95 |
0.92 |
0.09 |
0.05 |
0.13 |
0.05 |
0.86 |
0.86 |
|
Model
4 (gl: 9) |
15.51 |
0.97 |
0.95 |
0.06 |
0.02 |
0.1 |
0.05 |
0.85 |
0.85 |
Note. N = 182. Model 1 = original
one-factor model. Model 2 = model allowing correlated residuals between items 1
and 3. Model 3 = one-factor model excluding item 1. Model 4 = one-factor model
excluding item 3 but retaining item 1. CI = Confidence Interval.
We tested two additional exploratory
models: a six-item model excluding Item 1 (Model 3) and a six-item model
retaining Item 1 but excluding Item 3 (Model 4). Among these, Model 4
demonstrated the best fit indices (Table 3). However, because eliminating Item
3 could not be theoretically justified, we selected the one-factor model with a
correlated error between Items 1 and 3 (Model 2) as the final solution. The
internal consistency of this model was adequate (ω = 0.87).
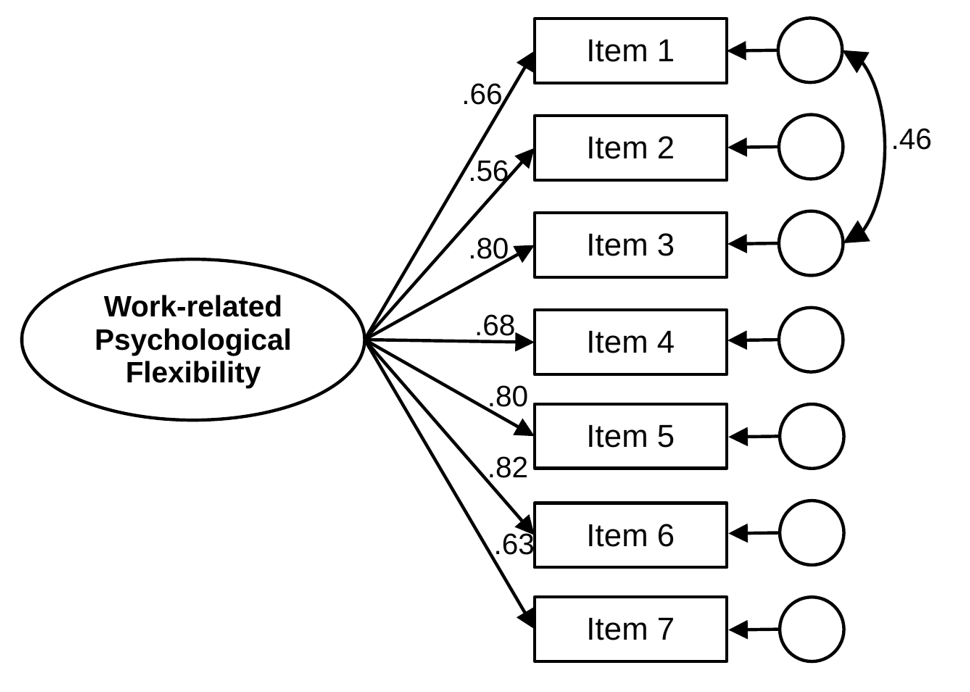
Figure 1. Confirmatory Factor Analysis of the Work-Related Acceptance and Action
Questionnaire.
Associations With Other Variables
Regarding
correlations with external variables, psychological flexibility as measured by
the WAAQ was negatively associated with depression, showing a small-to-moderate
correlation (rs = -0.28, 95% CI [-0.41,
-0.14], p < 0.001), and with anxiety, showing a moderate correlation (rs = -0.30, 95% CI [-0.42, -0.16], p <
0.001).
DISCUSSION
The present study examined the psychometric properties
of the WAAQ in healthcare professionals. Results indicated that a one-factor
model with a correlated residual between Items 1 and 3 provided the best fit.
As expected, WAAQ scores were associated with anxiety and depression in the
predicted directions.
It is worth noting that, unlike previous studies using
the WAAQ (Holmberg et al., 2019; Ruiz & Odriozola-González, 2014; Xu et
al., 2018), the present research employed confirmatory factor analysis (CFA).
This represents an advantage, as CFA allows a more stringent test of
dimensionality, thereby providing stronger validity evidence for the scale's
structure (Furr, 2018). In addition, we estimated internal consistency using
coefficient omega, which is considered more appropriate for psychological measures
that may not meet the assumption of tau-equivalence (Dunn et al., 2014;
McNeish, 2018). Indeed, current recommendations favor coefficient omega over
traditional Cronbach's alpha (Viladrich et al., 2017).
The findings further showed that psychological
flexibility was negatively and moderately correlated with depression and
anxiety. Previous research has consistently documented associations between
psychological flexibility and diverse psychological problems (Aguirre-Camacho
& Moreno-Jiménez, 2017). Moreover, within the healthcare context,
psychological flexibility has been linked to specific occupational phenomena
such as burnout (Ortiz-Fune, 2019). Taken together, these findings underscore
the relevance of psychological flexibility in explaining both emotional
problems and work-related difficulties, suggesting that future studies should
continue to incorporate measures of this process. For instance, other
instruments, such as the Emotional Acting at Work Scale (Salessi
& Omar, 2016), may be helpful to expand the assessment of psychological
flexibility in occupational contexts.
Limitations and strengths
Several limitations of the present study should be
acknowledged. First, the sample was convenience-based and included only
professionals who voluntarily participated in the online survey. This method
introduces potential self-selection bias, as participation was restricted to
individuals with digital access and sufficient motivation to complete the form,
potentially excluding healthcare workers with limited connectivity or those
under extreme work pressure. Therefore, the results may not be generalizable to
all healthcare professionals in Peru. For example, the majority of participants
were psychologists, which likely reflects the authors' professional networks.
Similarly, other sociodemographic characteristics may not represent the target
population.
Furthermore, data collection occurred at the beginning
of the third year of the COVID-19 pandemic; replication across different
contexts will be important. Second, the study did not include additional
work-related variables (e.g., job satisfaction). Future research should examine
whether WAAQ scores significantly predict outcomes relevant to occupational
well-being. Third, although a pair of correlated errors between WAAQ Items 1
and 3 was theoretically justified (semantic overlap in private events within the
ACT framework), this post hoc modification may increase the risk of overfitting
(Domínguez-Lara, 2019); future studies should cross-validate this model in
independent samples. Finally, although invariance testing would be valuable for
evaluating the stability of the factor structure, particularly the
correlated-error model, the sample size falls short of the minimum requirements
for reliable invariance analysis (Putnik & Bornstein, 2016). Despite these
limitations, this study contributes by examining the functioning of the WAAQ in
a new population using statistical methods not applied in prior research.
Conclusions
The present findings suggest that the WAAQ is an
appropriate measure of work-related psychological flexibility among healthcare
professionals. Replication studies in other samples and with additional
variables of interest will further strengthen its evidence base.
ORCID
Jesus Blancas-Guillen: https://orcid.org/0000-0002-9106-8072
Leandra Ccoyllo-Gonzalez: https://orcid.org/0000-0003-2366-5171
Giuliana Salazar-Alvarez: https://orcid.org/0000-0002-1387-8707
Franco Andree Méndez-Flores: https://orcid.org/0009-0000-6667-4532
Pablo D. Valencia: https://orcid.org/0000-0002-6809-1805
AUTHORS’ CONTRIBUTION
Jesus Blancas-Guillen:
Conceptualization; Writing - Original Draft; Project administration
Leandra
Ccoyllo-Gonzalez: Conceptualization; Writing - Original Draft; Project
administration
Giuliana
Salazar-Alvarez: Conceptualization; Writing - Original Draft; Writing - Review
& Editing
Franco Andree
Méndez-Flores: Formal analysis; Writing - Original Draft
Pablo D. Valencia:
Data Curation; Writing - Review & Editing
FUNDING
SOURCE
This study was self-funded.
CONFLICT
OF INTEREST
The authors declare that there were no
conflicts of interest in the collection of data, analysis of information, or
writing of the manuscript.
ACKNOWLEDGMENTS
Not applicable.
REVIEW
PROCESS
This study has been reviewed by two external reviewers in double-blind
mode. The editor in charge was David Villarreal-Zegarra. The review process is included
as supplementary material 1.
DATA AVAILABILITY
STATEMENT
The authors
attach the database as supplementary material 2.
DECLARATION OF THE USE OF GENERATIVE ARTIFICIAL INTELLIGENCE
We used DeepL to translate specific sections
of the manuscript and Grammarly to improve the wording of certain sections. The
final version of the manuscript was reviewed and approved by all authors.
DISCLAIMER
The authors are responsible for all statements made in this article.
REFERENCES
Aguirre-Camacho, A., & Moreno-Jiménez, B. (2017). La relevancia de
la flexibilidad psicológica en el contexto del cáncer: Una revisión de la
literatura [The relevance of
psychological flexibility
in the context of cancer: A literature
review]. Psicooncología, 14(1),
11–22. https://doi.org/10.5209/PSIC.55808
Barrett, K., & Stewart, I. (2021). A preliminary comparison of the
efficacy of online Acceptance and Commitment Therapy (ACT) and Cognitive Behavioural Therapy (CBT) stress management interventions
for social and healthcare workers. Health & Social Care in the Community,
29(1), 113–126. https://doi.org/10.1111/hsc.13074
Biglan, A., & Hayes, S. C. (1996). Should the behavioral sciences become
more pragmatic? The case for functional contextualism in research on human
behavior. Applied and Preventive Psychology, 5(1), 47–57. https://doi.org/10.1016/S0962-1849(96)80026-6
Bond, F. W., & Bunce, D. (2003). The role of acceptance and job
control in mental health, job satisfaction, and work performance. Journal of
Applied Psychology, 88(6), 1057–1067. https://doi.org/10.1037/0021-9010.88.6.1057
Bond, F. W., & Flaxman, P. E. (2006). The ability of psychological
flexibility and job control to predict learning, job performance, and mental
health. Journal of Organizational Behavior Management, 26(1–2),
113–130. https://doi.org/10.1300/J075v26n01_05
Bond, F. W., Flaxman, P. E., & Bunce, D. (2008). The influence of
psychological flexibility on work redesign: Mediated moderation of a work
reorganization intervention. Journal of Applied Psychology, 93(3),
645–654. https://doi.org/10.1037/0021-9010.93.3.645
Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. M., Guenole, N., Orcutt, H. K., Waltz, T., & Zettle, R. D.
(2011). Preliminary psychometric properties of the Acceptance and Action
Questionnaire–II: A revised measure of psychological inflexibility and
experiential avoidance. Behavior Therapy, 42(4), 676–688. https://doi.org/10.1016/J.BETH.2011.03.007
Bond, F. W., Lloyd, J., & Guenole, N.
(2013). The Work-related Acceptance and Action Questionnaire: Initial
psychometric findings and their implications for measuring psychological
flexibility in specific contexts. Journal of Occupational and Organizational
Psychology, 86(3), 331–347. https://doi.org/10.1111/joop.12001
Bravo, D. M., Falcón, J. C. S., Salguero, J. M. B., Luciano, B. G.,
& Ruiz, F. J. (2023). Psychometric
properties and measurement invariance of the Work-Related Acceptance and Action
Questionnaire (WAAQ) in a Colombian sample. International Journal of
Psychology & Psychological Therapy, 23(3), 301–312.
Dominguez-Lara, S. (2019). Correlation between residuals in confirmatory
factor analysis: a brief guide to their use and interpretation. Interacciones, 5(3),
e207. https://doi.org/10.24016/2019.v5n3.207
Dunn, T. J., Baguley, T., & Brunsden, V.
(2014). From alpha to omega: A practical solution to
the pervasive problem of internal consistency estimation. British Journal of
Psychology, 105(3), 399–412. https://doi.org/10.1111/bjop.12046
Ferrando, P. J., & Anguiano-Carrasco, C. (2010). El análisis factorial como técnica de investigación en psicología
[Factor analysis as a research
technique in psychology]. Papeles
del Psicólogo, 31(1), 18–33.
Fumero, A., & Navarrete, G. (2016). Personalidad y malestar
psicológico: Aplicación de un modelo de redes neuronales [Personality
and psychological distress:
Application of a neural network model]. Revista
Iberoamericana de Diagnóstico y Evaluación Psicológica, 41(1),
28–38.
Furr, R. M. (2018). Psychometrics: An
introduction (3rd ed.). SAGE.
Gaupp, R., Walter, M., Bader, K., Benoy, C., & Lang, U. E. (2020). A two-day Acceptance and Commitment Therapy (ACT) workshop increases
presence and work functioning in healthcare workers. Frontiers in Psychiatry,
11, 861. https://doi.org/10.3389/fpsyt.2020.00861
Hayes, S. C. (2004). Acceptance and commitment therapy, relational frame
theory, and the third wave of behavioral and cognitive therapies. Behavior
Therapy, 35(4), 639–665. https://doi.org/10.1016/S0005-7894(04)80013-3
Hayes, S. C., Barnes-Holmes, D., & Roche, B. (Eds.). (2001). Relational
Frame Theory: A post-Skinnerian account of human language and cognition.
Plenum Press.
Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A., & Lillis, J.
(2006). Acceptance and Commitment Therapy: Model, processes and outcomes. Behaviour Research and Therapy, 44(1),
1–25. https://doi.org/10.1016/J.BRAT.2005.06.006
Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2014). Terapia de
aceptación y compromiso: Proceso y práctica del cambio consciente (Mindfulness)
[Acceptance and Commitment Therapy: The process and practice of mindful change].
Desclée de Brouwer.
Hayes, S. C., Wilson, K. G., Gifford, E. V., Follette, V. M., &
Strosahl, K. (1996). Experiential avoidance and behavioral disorders: A
functional dimensional approach to diagnosis and treatment. Journal of
Consulting and Clinical Psychology, 64(6), 1152–1168. https://doi.org/10.1037/0022-006X.64.6.1152
Holmberg, J., Kemani, M. K., Holmström, L., Öst, L.-G., & Wicksell, R.
K. (2019). Evaluating the psychometric characteristics of
the Work-related Acceptance and Action Questionnaire (WAAQ) in a sample of
healthcare professionals. Journal of Contextual Behavioral Science, 14,
103–107. https://doi.org/10.1016/j.jcbs.2019.08.010
Kashdan, T. B., Barrios, V., Forsyth, J. P., & Steger, M. F. (2006).
Experiential avoidance as a generalized psychological vulnerability:
Comparisons with coping and emotion regulation strategies. Behaviour
Research and Therapy, 44(9), 1301–1320.
https://doi.org/10.1016/j.brat.2005.10.003
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2003). The
Patient Health Questionnaire-2: Validity of a two-item depression screener. Medical
Care, 41(11). https://doi.org/10.1097/01.MLR.0000093487.78664.3C
Kroenke, K., Spitzer, R. L., Williams, J. B. W., Monahan, P. O., &
Löwe, B. (2007). Anxiety disorders in primary care: Prevalence, impairment,
comorbidity, and detection. Annals of Internal Medicine, 146(5), 317–325. https://doi.org/10.7326/0003-4819-146-5-200703060-00004
Leal-Soto, F., Cuadros, O., Ortiz-Iñíguez, N., & Zenteno-Osorio, S.
(2022). Desarrollo y evidencia de validez de constructo de un instrumento para
evaluar experiencia escolar [Development and construct validity evidence of an
instrument to assess school experience].
Revista Iberoamericana de Diagnóstico y Evaluación Psicológica, 63(2),
147–162. https://doi.org/10.21865/RIDEP63.2.11
Lloret-Segura, S., Ferreres-Traver, A.,
Hernández-Baeza, A., & Tomás-Marco, I. (2014). Exploratory item factor analysis: A practical guide revised and updated.
Anales de Psicología, 30(3), 1151–1169. https://doi.org/10.6018/analesps.30.3.199361
Luciano, C., & Hayes, S. C. (2001). Trastorno de evitación
experiencial [Experiential avoidance
disorder]. International Journal of Clinical and Health Psychology, 1(1), 109–157.
McNeish, D. (2018). Thanks coefficient alpha, we’ll take it from here. Psychological
Methods, 23(3), 412–433. https://doi.org/10.1037/met0000144
Ortiz-Fune, C. (2019). Burnout como inflexibilidad psicológica en profesionales sanitarios: Revisión y nuevas propuestas de intervención desde una perspectiva contextual-funcional [Burnout as psychological inflexibility in
healthcare professionals: Review and new intervention proposals from a
contextual-functional perspective]. Apuntes de Psicología, 36(3),
135–144. https://doi.org/10.55414/8jfbsa09
Paniagua, D., Alvarado, J. M., Olivares, M., Ruiz, I., Romero-Suárez,
M., & Aguayo-Estremera, R. (2022). Estudio de seguimiento de las
recomendaciones sobre análisis factorial exploratorio en RIDEP [Follow-up study of recommendations on exploratory factor analysis in RIDEP]. Revista Iberoamericana de
Diagnóstico y Evaluación Psicológica, 66(5), 127–139. https://doi.org/10.21865/RIDEP66.5.10
Persons, J. B., Fresco, D. M., & Ernst, J. S. (2018). Adult depression. In J. Hunsley & E. J. Mash (Eds.), A guide to
assessments that work (pp. 131–151). Oxford University Press.
Ponce, M. C., & Villar, E. (2022). Validation of the Work-related
Acceptance and Action Questionnaire (WAAQ) with university students. Behavioral Psychology, 30(1),
223–233. https://doi.org/10.51668/bp.8322111s
Putnick, D. L., & Bornstein, M. H. (2016). Measurement invariance conventions and reporting: The state of the art
and future directions for psychological research. Developmental Review, 41,
71-90. https://doi.org/10.1016/j.dr.2016.06.004
Prudenzi, A., Graham, C. D., Clancy, F., Hill, D., O’Driscoll, R., Day,
F., & O’Connor, D. B. (2021). Group-based acceptance and commitment therapy
interventions for improving general distress and work-related distress in
healthcare professionals: A systematic review and meta-analysis. Journal of
Affective Disorders, 295, 192–202. https://doi.org/10.1016/j.jad.2021.07.084
Rhemtulla, M., Brosseau-Liard, P. É., & Savalei, V.
(2012). When can categorical variables be treated as continuous? A comparison
of robust continuous and categorical SEM estimation methods under suboptimal
conditions. Psychological Methods, 17(3), 354–373
Roemer, L., & Orsillo, S. M. (2005). An acceptance-based behavior
therapy for generalized anxiety disorder. In S. M. Orsillo & L. Roemer
(Eds.), Acceptance and mindfulness-based approaches to anxiety (pp.
213–240). Springer. https://doi.org/10.1007/0-387-25989-9_9
Ruiz, F. J., & Odriozola-González, P. (2014). The Spanish version of the Work-related Acceptance and Action
Questionnaire (WAAQ). Psicothema, 26(1),
63–68. https://doi.org/10.7334/psicothema2013.110
Salessi, S., & Omar, A. (2016). Desarrollo y validación de una
escala para medir actuación emocional en el trabajo [Development
and validation of a scale to measure
emotional acting at work]. Revista Iberoamericana de Diagnóstico y
Evaluación Psicológica, 41(1), 66–79.
Savalei, V., & Reise, S. P. (2019). Don’t forget the model in your model-based reliability coefficients: A
reply to McNeish (2018). Collabra: Psychology, 5(1),
36. https://doi.org/10.1525/collabra.247
Valiente-Barroso, C., Sáiz-Obeso, J.,
Valiente-Barroso, B., Lombraña-Ruiz, R., &
Martínez-Vicente, M. (2021). Inflexibilidad psicológica gestionada por
profesionales sanitarios durante el estado de alarma vinculado al COVID-19 [Psychological inflexibility managed by healthcare
professionals during the COVID-19 state of emergency]. Apuntes de
Psicología, 38(3), 149–158. https://doi.org/10.55414/ap.v38i3.821
Viladrich, C., Angulo-Brunet, A., & Doval, E. (2017). A journey around alpha and omega to estimate internal consistency
reliability. Anales de Psicología, 33(3), 755–782. https://doi.org/10.6018/analesps.33.3.268401
Wilson, K. G., & Luciano, C. (2002). Terapia de aceptación y
compromiso: Un tratamiento conductual orientado a los valores [Acceptance and commitment therapy: A behavioral therapy oriented to values]. Pirámide.
Xu, X., Liu, X., Ou, M., Xie, C., & Chen, Y. (2018). Psychological flexibility of nurses in a cancer hospital: Preliminary
validation of a Chinese version of the Work-related Acceptance and Action
Questionnaire. Asia-Pacific Journal of Oncology Nursing, 5(1),
83–90. https://doi.org/10.4103/apjon.apjon_62_17
Yuan, K.-H., & Bentler, P. M. (2000). Three likelihood-based methods for mean and covariance structure
analysis with nonnormal missing data. Sociological Methodology, 30(1), 165–200. https://doi.org/10.1111/0081-1750.00078