http://dx.doi.org/10.24016/2020.v6n3.171
ORIGINAL ARTICLE
Adaptation of the Beck Anxiety Inventory
in population of Buenos Aires
Adaptación del
Inventario de Ansiedad de Beck en población de Buenos Aires
Nicolás
Alejandro Vizioli 1 *, Alejandro Emilio Pagano 1
1 Universidad de Buenos Aires, Faculty of
Psychology, Argentina.
* Correspondence: nicovizioli@gmail.com.
Received: July 02, 2020 | Revised:
September 08, 2020 | Accepted: September
13, 2020 | Published Online:
September 14, 2020.
CITE IT AS:
Vizioli, N. & Pagano, A. (2020). Adaptation of the
Beck Anxiety Inventory in population of Buenos Aires. Interacciones, 6(3), e171.https://doi.org/10.24016/2020.v6n3.171
ABSTRACT
Background: Currently, anxiety disorders are the most
prevalent worldwide, reaching a rate of 5% in Argentina in 2017. The Beck
Anxiety Inventory (BAI) is one of the instruments most used in research and
clinic today. In its construction, one of the objectives was to evaluate
anxiety symptoms that are not usually evident in depressive disorders, which is
why it is a relevant test to make a differential diagnosis. The objective of
this study was to adapt the BAI to adult population of Buenos Aires. Methods: A direct translation of the
inventory and then an expert judgment to assess the content validity were
carried out. The discrimination capacity of the items was analyzed, and the
structural validity of the test were evaluated according to different models
found in the literature. Also, the internal consistency of the instrument was
analyzed. Results: The adaptation
presents adequate content validity and the items have been shown to
discriminate adequately. As for the confirmatory factor analyzes, the most
parsimonious solution, which indicates the one-dimensionality of the construct,
was chosen, providing evidence of construct validity. The adaptation presents
adequate internal consistency. Tentative normative values are offered. Conclusion: Evidence of validity and
reliability has been found for the Argentine adaptation of the BAI. It is
considered an instrument of great clinical utility.
Keywords: BAI; Anxiety; Population of Buenos Aires; Content validity; Construct
validity; Internal consistency.
RESUMEN
Introducción: En la actualidad
los trastornos de ansiedad son los de mayor prevalencia a nivel mundial,
llegando a una tasa del 5% en Argentina en el año 2017. En ese sentido, el
Inventario de Ansiedad de Beck (BAI) es uno de los instrumentos más utilizados
en investigación y clínica en la actualidad. En su construcción uno de los
objetivos fue evaluar síntomas de ansiedad que no suelen evidenciarse en
trastornos depresivos, motivo por el cual resulta un test relevante para
realizar un diagnóstico diferencial. El objetivo de este estudio fue adaptar el
BAI a población adulta de Buenos Aires.
Método: Se realizó una traducción directa del inventario y luego un juicio
de expertos para evaluar la validez de contenido. Se analizó la capacidad de
discriminación de los reactivos y se evaluó la validez estructural de los
diferentes modelos encontrados en la literatura. A su vez, se analizó la
consistencia interna del instrumento.
Resultados: La adaptación presenta adecuada validez de contenido y los
reactivos han demostrado discriminar de forma adecuada. A su vez, a partir de
los análisis factoriales confirmatorios realizados se optó por la solución más
parsimoniosa que indica la unidimensionalidad del constructo aportando evidencia
de validez de constructo. A su vez, la adaptación presenta una adecuada
consistencia interna. Se ofrecen valores normativos tentativos. Conclusión: Se han hallado evidencias
de validez y confiablidad para la adaptación argentina del BAI. Se lo considera
un instrumento de gran utilidad clínica.
Palabras clave: BAI; Ansiedad; Población de Buenos Aires; Validez de Contenido;
Validez de Constructo; Consistencia Interna.
BACKGROUND
Anxiety disorders are ranked as the most
prevalent disorders worldwide (Ritchie & Roser, 2018). In Argentina,
anxiety disorders constitute the group with the highest prevalence, followed by
mood disorders (Stagnaro et al., 2017). The relationship between both disorders
has been well documented in the research literature. Even the similarity of
symptoms between anxiety and depressive disorders can make investigation,
diagnosis and treatment difficult (Mountjoy and Roth, 1982). This problem can
be explained due to the cognitive biases shared by both pathologies, as well as
their frequent comorbidity. In this sense, cognitive biases in judgment and
interpretation of situations are common for both disorders, as well as
predominantly negative affection (Mineka, Watson & Clark, 1998).
In relation to the
comorbidity between anxiety and depressive disorders, it has been found that a
large part of people with anxiety disorders also experience depressive
disorders, and vice versa (Gorman, 1996). Even transdiagnostic treatments have
been developed that allow working with both problems, as is the case with the
unified protocol proposed by Barlow et al. (2016). This protocol is
characterized by addressing the common mechanism underlying both disorders:
emotional regulation. In this regard, it has been found that maladaptive
emotional regulation strategies can be common processes across various
psychological disorders (Aldao et al., 2010).
Also, calamitous events such as natural
disasters or attacks can cause a substantial increase in anxiety symptoms
(Clark & Beck, 2011). In 2020, different countries of the world have been
affected by the COVID-19 pandemic. The psychological impact caused by this
situation has caused an increase in anxiety and depressive symptoms (Rajkumar,
2020).
In this context, the evaluation and
follow-up of the problems associated with anxiety is fundamental, given that
they impose a great individual and social burden, tend to be chronic and can be
disabling (Lépine, 2002). Accordingly, it has been found that anxiety and
depression disorders involve a large part of the economic resources destined to
the treatment of psychological disorders (Ruiz-Rodríguez, 2017). However, it
has been estimated that only a quarter of the people who meet the criteria for
anxiety disorders have received treatment (Alonso et al., 2018).
Due to the aforementioned, it is necessary
to have valid and reliable instruments that allow a correct measurement of
anxiety and can discriminate these pictures from depressive disorders. In this
sense, the Beck Anxiety Inventory (BAI;Beck et al., 1988) was designed with a double
objective: to measure anxiety in a valid and reliable way and to discriminate
anxiety from depression (Sanz & Navarro, 2003). This anxiety assessment
instrument is also the most cited in scientific databases (Piotrowski, 2018),
as well as one of the most used in clinical and non-clinical populations both
in psychotherapeutic practice and in research (Magán et al., 2008).
For this reason, the
general objective of this research was to carry out the conceptual, linguistic
and metric adaptation of the Beck Anxiety Inventory in the general adult
population of the City of Buenos Aires and the Greater Buenos Aires. In this
way, the specific objectives proposed were a) to examine evidence of content
validity; b) analyze the discrimination capacity of the items; c) obtain
evidence of structural and construct validity; d) study the internal consistency
of scores; e) establish normative values.
METHODS
Participants
The sampling was non-probabilistic and
intentional. The sample consisted of 269 subjects, of which 49.4% resided in
the Autonomous City of Buenos Aires and 50.60% in the Province of Buenos Aires.
In relation to gender, 37.5% were male, 60.6% female, and 1.9% preferred not to
communicate it. Regarding the age of the participants, there were cases between
18 and 76 years (M = 32.35, SD = 12.17). Regarding educational level, 1.5%
presented complete primary school, 57.5% completed secondary school and 41%
reported having completed university studies. Finally, it was consulted whether
they had been diagnosed with any psychological problems, 86.2% reported not
being diagnosed, 7.1% mentioned being diagnosed with an anxiety disorder, 3.3%
depression and the remaining 3.4% other problems such as post-traumatic stress,
eating and personality disorders.
Instruments
First,
a sociodemographic questionnaire was designed to collect information on the
place of residence, age, gender, educational level, and history of
psychological diagnoses.
Second, the Spanish translated version of
the Beck Anxiety Inventory (BAI, Beck, Epstein, Brown & Steer, 1988) was
used. This inventory presents 21 items with a format designed to assess the
severity of clinical anxiety symptoms. Each BAI item reflects an anxiety
symptom and for each one, respondents rate the degree to which they were
affected by it during the last week, on a 4-point Likert scale, ranging from 0
(Not at all) to 3 (Severely - I get very upset). Regarding the score, each item
is assigned from 0 to 3 points, depending on the response of the individual
and, after directly adding the score for each item, a total score can be
obtained, ranging from 0 to 63.
Process
The
collection of analysis units was carried out through the use of virtual
platforms. An informed consent was included in which the details of the
objectives of the present investigation were specified, together with the
guarantees of confidentiality and anonymity. It was explained to the
participants that they could desist from participating at the moment they
considered it and in turn they were given an email to communicate in case they
felt discomfort when answering the questionnaire.
Data analysis
First, the translation
of the inventory was carried out according to the recommendations of Muñiz et
al. (2013), using the direct translation method in order to find linguistic and
cultural equivalence. Three bilingual experts with experience in instrument
translation were asked to each carry out a direct translation of the
questionnaire from English to Spanish. Once the three versions were obtained in
Spanish, a committee of experts was convened that could analyze the
translations made, in this way the most appropriate translations in linguistic
and cultural terms were then selected.
The expert trial
(Andreani, 1975) was carried out following the recommendations of Escobar-Pérez
and Cuervo-Martínez (2008). The criteria for selecting these judges were: a)
previous experience in conducting judgement of experts b) expert in
psychometrics and psychological evaluation c) knowledge on psychopathology e)
knowledge about construct anxiety. Once the five expert
judges were selected, the instructions and forms were prepared to be provided
by mentioning the objectives of the study and the slogan regarding the trial
they were expected to conduct. To assess semantic and syntactic clarity, expert
judges used a four-point likert scale where 1 indicated "different",
2 "quite different" 3, "pretty similar" and 4
"identical", this referred to whether the reagent was easily
understood, in our cultural context. On the other hand, to assess the
consistency of translations, expert judges used a four-point likert scale where
1 indicated "does not meet the criterion", 2 "low
level" 3, "moderate level" and 4 "high level", this referred to thus the reagent makes sense with respect to the
dimension or indicator it is measuring. Finally, to assess the relevance of
translations, expert judges used a four-point likert scale where 1 indicated
"does not meet the criterion", 2 "low level"
3, "moderate level" and 4 "high level", this referred to thus the reagent was essential or very important and
should be excluded.
Through these scales, each expert
responded by reading the item from the original version and then scored each of
the three translations establishing the semantic equivalence, coherence and
relevance of the items. according to the recommendations of Tornimbeni et al. (2008). In this way, the final version was made
up of the items that obtained the highest score by the judges. In turn, an
observations section was established, instructing the judge to make
observations regarding the congruence of the item with the dimension and syntactic
aspects that he wanted to highlight.
Once the results of each
of the judges were obtained, a form was made with all the valuations from which
the percentage of agreement was estimated (Tinsley and Weiss, 1975) and the
coefficient V of Aiken (Aiken, 1985) of the trial carried out by all judges.
These agreement indicators are represented by values ranging from 0 to 1 the
closer to 1 the reagent will have greater content validity.
Second, according to the
recommendations of Hogan (2004), a discrimination analysis of the items was
carried out, providing information on the ability of an item to differentiate
in statistical terms the individuals who have a higher value of the variable of
those who have a lower level. The internal method of comparison between
extremes was used (Muñiz, 2005), dividing the sample into quartiles with
respect to the total score obtained. Once this was done, a comparison was made
of the values of each item in the two groups –quartile 1 and quartile 4-,
thus determining which items discriminate adequately. To do this, the Mann
Whitney U statistic was used, since the items did not fulfill the assumption of
normality.
Third, the structural
validity of the BAI was evaluated. For this, three models disseminated in the
literature were tested: the one-factor (Magán et al., 2008), the original
two-factor (Beck et al., 1988), and the four-factor (Osman et al., 1993).
Because the data did not meet the normality criteria and the response format of
the BAI, following the criteria adopted by Osman et al. (1997), an analysis of
the covariance matrices was carried out using the elliptical test with
reweighted least squares (Browne, 1984) with the EQS version 6.1 statistical
software.
The following goodness
of fit indices were considered: x2 divided by the degrees of freedom
(values ≤ 5.0 indicate a good fit); NNFI (Non-Normed Fit Index); CFI
(Comparative Fit Index), RMSEA (Root Mean Square Error of Approximation) and
SRMR (Standardized Root Mean-Square Residual). According to the criteria
specified by Kline (2011) and Schumacker & Lomax (2016), values greater
than or equal to .90 in NNFI and CFI and values less than or equal to .06 in
RMSEA and less than .08 in RMSEA and less than .08 in SRMR. In turn, the AIC
(Akaike's Information Criterion) was taken into account, which yields relative
values. The best model will be the one with the lowest AIC. The construct
validity was evaluated by examining the factor loadings. Values above .30
were considered adequate (Nunnally & Bernstein, 1994).
Finally, to assess
internal consistency, the α ordinal and ω ordinal reliability
indices were calculated (McDonald, 1999), from polychoric correlation matrices.
For this, the R program version 3.6.0 and the following R packages were used:
GPArotation (Bernaards, & Jennrich, 2005), psych (Revelle, 2018) and Rcmdr
(Fox, & Bouchet-Valat, 2019). The composite reliability coefficient ρ (Bentler, 1968) was
also reported, based on the standardized loads of the items that make up the
inventory. In turn, the corrected item-factor correlations were calculated,
considering as adequate values greater than .40. (Nunnally & Bernstein,
1994).
To establish normative
values, percentile scores were calculated with the SPSS version 26 software, in
accordance with the recommendations of Sanz (2014).
Ethical aspects
The purpose of the
study was explained in writing before administration began. All participants
gave their consent. Informed consent set out the characteristics of the
participation, which was anonymous, voluntary and uncompensated. At the end of
the administration, participants were provided with the document containing the
recommendations to face the pandemic, published by the Faculty of Psychology of
the University of Buenos Aires (2020).
RESULTS
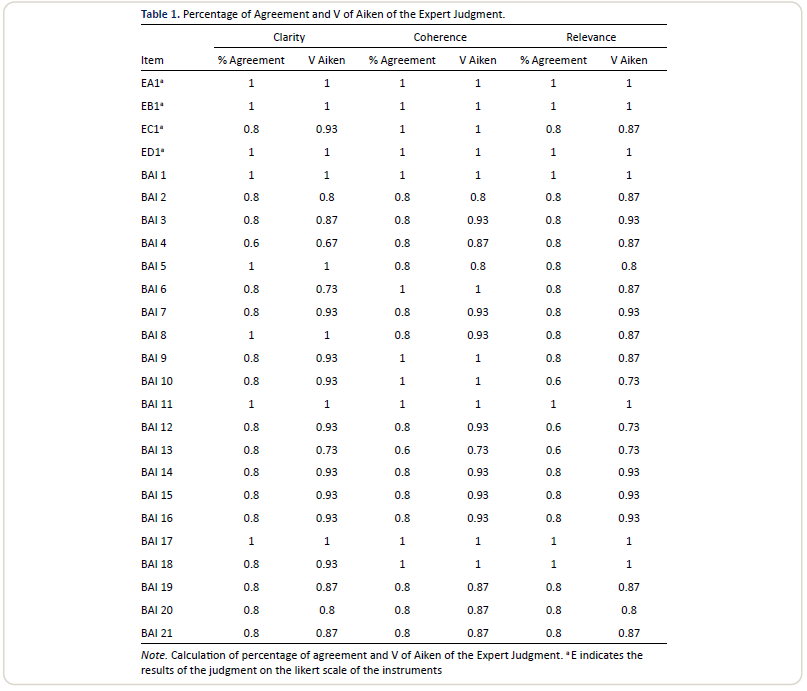
To obtain evidence of
content validity, the expert judgment was conducted. From the three
translations and the indications of the five judges, the 21 items were
selected. Regarding the three established criteria -Semantic equivalence, coherence and relevance- the
items that made up the final version, obtained percentages of agreement between
.80 and 1, adequate according to the literature (Voutilainen & Liukkonen,
1995, cited in Hyrkäs et al., 2003) with the exception of item 4 -Unable to
relax- whose semantic clarity index was below .80, its translation was
“Inability to relax”. In this particular item, one of the judges questioned
whether it was written in the first person. Based on this observation, it was
decided to modify the item so that the final version ended up being
"Inability to relax."
In turn, Aiken's V
coefficients ranged between values of .80 to1 mostly, acceptable values
according to the literature (Aiken, 2003). However, items 4, 6, 10 and 13
values were not adequate (see table 1). Regarding item 4, the modification
that was made based on the evaluations and observations has already been
indicated. In item 6 -Dizzy or lightheaded- whose final translation was
"Dizziness or vertigos" the translation brought difficulties due to
the low frequency of the words translated in our language, as no observations
were received from the judges, it was decided to consult a specialist in
linguistics from which it was decided to keep the aforementioned translation.
In relation to item 10 –Nervous- whose final translation was “Nervous”, as can
be seen in Table 1, the judges indicated disagreement regarding the relevance
of the item to assess anxiety symptoms, Due to the adaptation nature of the
present work, it was preferred to keep the item and evaluate its behavior at
the metric level. In turn, item 13 -Shaky / unsteady- whose translation was
“Restless / insecure” presented inadequate values regarding its clarity and
relevance. Based on the observations received by the judges, it was decided to
replace the word insecure with shaky, defining the final version of the item as
“Inquiero / shaky”. Finally, two of the expert judges reported that the DSM 5
(American Psychological Association, 2013) made a modification in the diagnosis
of panic disorder and the criterion "Fades or fainting" was modified
by "Feeling fainting or fainting" understanding that the test was
built under an earlier version of the DSM taking as a criterion that symptom
was decided to modify it by translating item 19 as Feeling of fading or
fainting.
In
conclusion, the expert trial has provided valuable results in relation to the
analysis and modification of direct translations by bilingual judges in such a
way that certain inconsistencies that were corrected or in some cases will be
taken into account in subsequent reagent analyses have been detected.
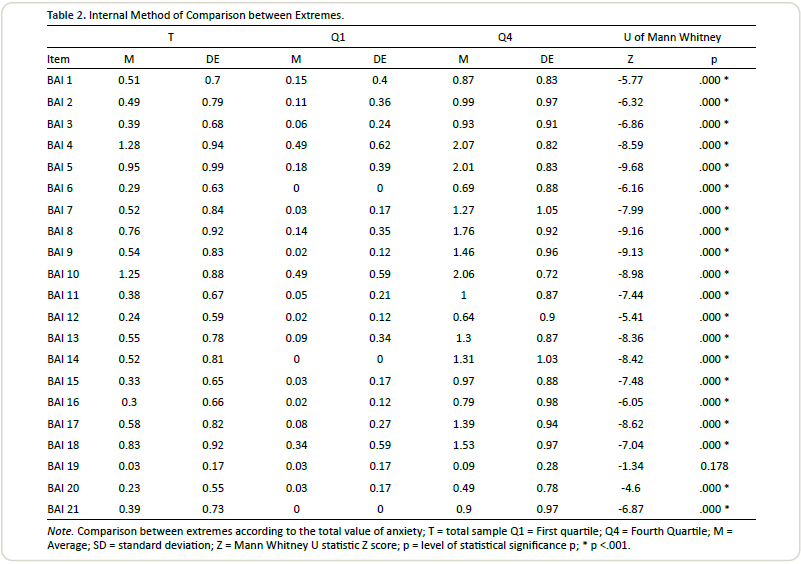
Regarding the analysis of the reagents,
Table 2 shows the results of the comparison of the items according to quartile
1 and quartile 4 obtained by the total score of each case. The differences were
significant in all cases p <.01 (α = .01), with the exception of item 19, this would
indicate that all of them discriminate adequately. Regarding item 19 - Feeling
of fainting or fainting - it should be noted that it only obtained responses of
1 and 2 points on the Likert scale in the entire sample. It is probable that
although the discrimination power of item 19 was not adequate, it has a
clinical utility at a qualitative level, for this reason, it was decided to
keep it and evaluate it from the confirmatory factor analysis carried out.
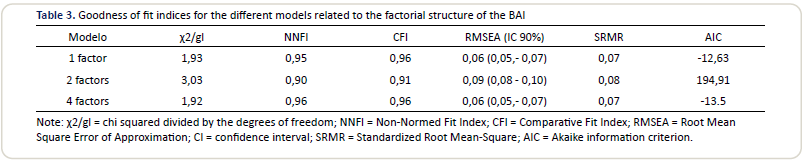
To examine the factorial structure, 3
models were tested: the one-factor, the original two-factor and the four-factor
models, through a confirmatory factor analysis performed from the analysis of
the covariance matrices using the elliptical test with minimums. reweighted
squares.
Regarding the single factor model, the
goodness of fit indices were the following: χ2 (184) =
355.37; CFI = 0.96; NNFI = 0.95; RMSEA = 0.06; SRMR = 0.07; AIC = -12.63.
Regarding the two-factor model, the goodness of fit indices obtained were: χ2 (188) = 570.91; CFI = 0.91; NNFI = 0.90; RMSEA = 0.09; SRMR = 0.08;
AIC = -194.91. In relation to the four-factor model, the following goodness of
fit indices were obtained: χ2 (183) = 352.96; CFI = 0.96; NNFI = 0.96;
RMSEA = 0.06; SRMR = 0.07; AIC = -13.05 (Table 3). These results indicate that
the most suitable model is that of a factor.
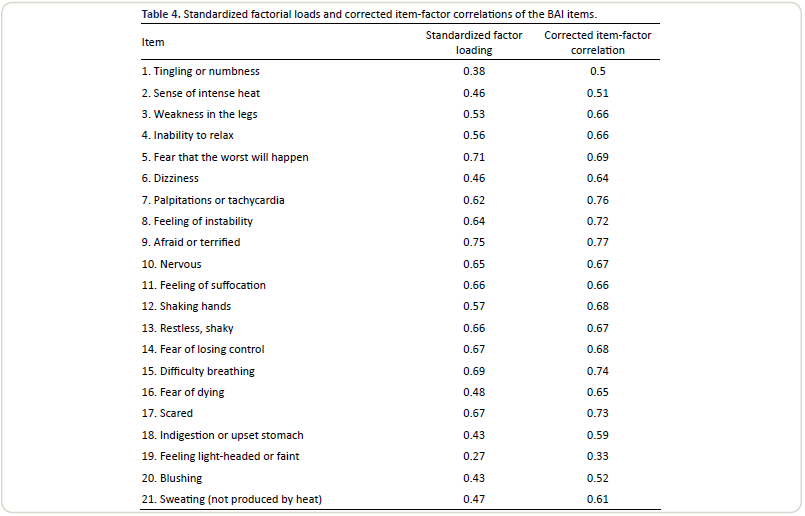
Regarding the construct validity, the
standardized factor loadings, scores greater than> .40 were obtained in all
cases except for item 19: “feeling of fainting or fainting”, whose standardized
load was 0.27 (Table 4).
In relation to internal consistency,
ordinal alpha and omega were calculated for the only factor that makes up the
entire inventory. Α ordinal = 0.93, ω ordinal =
0.95 were obtained. Regarding the composite reliability, ρ = 0.92 was obtained. The corrected item-factor correlations have been
obtained satisfactory values for all items except for item 27 (Table 4).
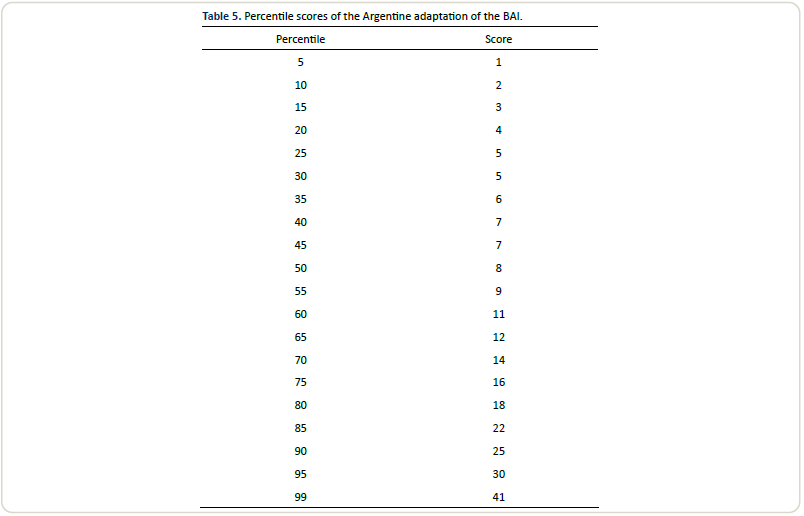
In relation to the formulation of
normative values, Table 5 provides percentile scores for the scores of the
Argentine adaptation of the BAI.
DISCUSSION
The general objective
of this research was to carry out the conceptual, linguistic and metric
adaptation of the Beck Anxiety Inventory in the general adult population of
Buenos Aires. The specific objectives proposed were a) to examine evidence of
content validity; b) analyze the discrimination capacity of the items; c)
obtain evidence of structural and construct validity; d) study the internal
consistency of scores; 3) establish normative values.
Following the
recommendations of Muñiz et al. (2013), it was decided to carry out a direct
translation of the questionnaire, the expert judges evaluated the semantic and
syntactic clarity of the adapted version. The process provided relevant
information to correct linguistic aspects in some cases –item 4- and cultural
ones where words more representative of the symptomatology in our culture were
used –items 6 and 13-. In turn, a modification was made to item 19 based on the
change produced in DSM 5. In the new version of the manual it is reported that
the diagnostic criteria for panic disorder, fainting, and dizziness are related
to the perception of loss of consciousness. control or death and it was
specified that the criterion should contemplate the sensation since it is
typical of the disorder that the person perceives that sensation and it does
not always become concrete (American Psychological Association, 2013). Due to
the aforementioned, item 19 "Fainting or fainting spells" was
modified for "Feeling of fainting or dizzy". The aforementioned
changes account for a translation process that included the updating and the
context of application of the instrument. On the other hand, the acceptable
values of percentage of agreement and V of Aiken in the relevance dimension,
evaluated by the expert judges, show that the adapted version presents adequate
content validity. In turn, the reliability coefficients that in all cases
exceed .90 provide greater evidence of the internal consistency presented by
the questionnaire. This indicates that the items are a representative sample of
the anxiety symptoms that the questionnaire intends to measure. However, item
10 has been questioned by the judges regarding the relevance to assess anxiety
symptoms, however, both the comparison test between extremes (which shows an
adequate discrimination power of the item) and the CFA where the item has a
high factorial load, show its relevance in the test. It would be appropriate to
evaluate the aforementioned items in tests of convergent and discriminant
validity.
On the other hand, with
the exception of item 19, the items have shown adequate discrimination power in
all cases, from separating the sample into quartiles based on the total score,
it was evidenced that the items discriminate adequately between those with
major and minor anxiety symptoms. Regarding item 19, as mentioned above, as it
is a specific item for panic disorder, it should be studied in a clinical
population in order to evaluate its discrimination power according to anxiety
disorder.
Regarding structural
validity, although the three models studied obtained adequate goodness-of-fit
indices, it was found that the best model is one factor. This result coincides
with the research of Magán et al., 2008, who when they adapted the instrument
in the Spanish population and found that the most appropriate solution was a
global anxiety factor. In this sense, the results are not coincident with the
original two-factor structure (Beck et al., 1988). In that sense, Bardhoshi, Duncan & Erford (2016), in a psychometric meta-analysis
on the properties of the English versions of the BAI, found that studies have
reported solutions of 1 to 6 factors. In such a way that population
peculiarities could affect the factorial structure of the instrument.
When analyzing the standardized loadings of the items, satisfactory
values were found in all cases, except again in item 19, "Feeling of
fainting or fainting." This result can be explained because the item
refers to a specific diagnostic criterion only for panic disorder for DSM 5. It is important to
clarify that other anxiety disorders can lead to panic episodes, which justifies
keeping the item as a relevant qualitative indicator is highlighted in the
final version of the Argentine adaptation of the inventory. However, it is recommended to analyze the psychometric properties of the inventory
in larger samples, as well as in the clinical population to reevaluate its
functioning.
Taking into account the fourth objective to study the internal
consistency of the scores, excellent values were obtained in the three
calculated indexes, according to the criterion established by George &
Mallery (2003): Ordinal α =0,93, ordinal ω = 0,95, and composite reliability
ρ=0,92.
Regarding the last objective, namely
establishing normative values, percentile scores obtained from the application
of the BAI are offered. Although these normative values can be indicative in
relation to the global level of anxiety, it is suggested to interpret them
carefully and take them as tentative. Given the small sample size and the
non-representativeness of the sample.
To conclude, the Argentine adaptation of
the Beck Anxiety Inventory is a valid and reliable instrument for the
evaluation of anxiety symptoms in adults in Buenos Aires. As it is a short and
easy-to-administer instrument, it is considered very useful for carrying out
follow-up tasks in the current context, as well as for evaluating
psychotherapeutic interventions.
Regarding the limitations of the study
carried out, first of all the small size and non-probabilistic nature of the
sample collected can be mentioned. Future research may take larger and more
representative samples, as well as from different regions of the country, to
have a global vision about the phenomenon of interest.
Secondly, even with the evidence obtained,
new studies are required to analyze factor constancy through different samples,
as well as convergent and discriminant validity. Specifically, to study the
discriminative power of BAI in relation to depressive symptoms.
Third, it is suggested that later studies
investigate invariance of different sociodemographic variables such as gender
or age, to ensure that the factorial structure is constant in different groups.
ORCID
Nicolas Alejandro
Vizioli https://orcid.org/0000-0002-6113-6847
Alexander Emilio
Paganohttps://orcid.org/0000-0003-4817-9145
AUTHORS
'CONTRIBUTION
Nicolás Alejandro Vizioli: Conceptualization, methodology, software,
validation, formal analysis, research, writing - original draft,
writing-review, visualization.
Alejandro Emilio Pagano: Conceptualization, methodology, software,
validation, formal analysis, data curation, writing - original draft,
visualization.
FUNDING
Self-funded research.
CONFLICT OF INTERESTS
The authors declare that there is no conflict of interest.
ACKNOWLEDGEMENTS
Does not apply.
REVIEW
PROCESS
This study has been peer-reviewed in a
double-blind manner.
DECLARATION
OF DATA AVAILABILITY
The authors express our support for open
science. However, we consider it relevant to safeguard the database to preserve
the anonymity of the participants and the confidentiality of the data, in
relation to professional secrecy. The database, as well as the instrument, may
be requested from the authors' emails.
DISCLAIMER
The authors are responsible
for all statements made in this article. Neither Interactions nor the Peruvian
Institute of Psychological Orientation are responsible for the statements made
in this document.
REFERENCES
Aiken,
L. R. (2003). Tests psicológicos y evaluación. Pearson educación.
Aiken, L. R. (1985).
Three coefficients for analyzing the reliability and validity of ratings [Tres
coeficientes para analizar la confiabilidad y validez de las calificaciones]. Educational and psychological measurement, 45(1), 131-142.
https://doi.org/10.1177/0013164485451012
Aldao, A.,
Nolen-Hoeksema, S., & Schweizer, S. (2010). Emotion-regulation strategies
across psychopathology: A meta-analytic review. Clinical psychology review, 30(2), 217-237.
https://doi.org/10.1016/j.cpr.2009.11.004
Alonso, J. et al (2018).
Treatment gap for anxiety disorders is global: Results of the World Mental
Health Surveys in 21 countries. Depression and anxiety, 35(3), 195-208. https://doi.org/10.1002/da.22711
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental
disorders (DSM-4®). Author.
American Psychiatric
Association. (2013). Diagnostic and
statistical manual of mental disorders (DSM-5®). American Psychiatric Pub.
Andreani, O. (1975). Aptitud Mental y Rendimiento Escolar. Herder.
Bardhoshi, G., Duncan, K., & Erford, B. T. (2016). Psychometric
meta‐analysis of the English version of the Beck Anxiety Inventory. Journal of Counseling & Development,
94(3), 356-373. https://doi.org/10.1002/jcad.12090
Barlow, D. H., Farchione, T. J., Fairholme, C. P., Ellard, K. K.,
Boisseau, C. L., Allen, L. B., & Ehrenreich-May, J. (2016). Protocolo unificado para el tratamiento transdiagnóstico de
los trastornos emocionales. Alianza Editorial.
Beck, A. T., Epstein, N., Brown, G., & Steer, R. A. (1988). An inventory for measuring
clinical anxiety: Psychometric properties [Un inventario para medir la ansiedad
clínica: propiedades psicométricas]. Journal
of Consulting and Clinical Psychology, 56(6),
893–897. https://doi.org/10.1037/0022-006X.56.6.893
Bentler, P. M. (1968).
Alpha-maximized factor analysis (alphamax): Its
relation to alpha and
canonical factor analysis. Psychometrika,
33,
335–345.
http://dx.doi.org/10.1007/BF02289328
Bentler, P. M. (1990).
Comparative fit indexes in structural models. Psychological bulletin, 107(2), 238. https://psycnet.apa.org/doi/10.1037/0033-2909.107.2.238
Bernaards, C. A., &
Jennrich, R. I. (2005). Gradient projection algorithms and software for
arbitrary rotation criteria in factor analysis. Educational and Psychological Measurement, 65, 676-696.
https://doi.org/10.1177/0013164404272507
Brown, T. A. (2006). Confirmatory factor analysis for applied
research. Guilford publications.
Browne, M. W. (1984).
Asymptotically distribution‐free methods for the analysis of covariance
structures. British journal of
mathematical and statistical psychology, 37(1), 62-83.
https://doi.org/10.1111/j.2044-8317.1984.tb00789.x
Clark, D. A., & Beck,
A. T. (2011). Cognitive therapy of
anxiety disorders: Science and practice. Guilford Press.
Escobar-Pérez, J., y
Cuervo-Martínez, Á. (2008). Validez de
contenido y juicio de expertos: una aproximación a su utilización. Avances
en medición, 6(1), 27-36. https://www.researchgate.net/profile/Jazmine_Escobar-Perez/publication/302438451_Validez_de_contenido_y_juicio_de_expertos_Una_aproximacion_a_su_utilizacion/links/59a8daecaca27202ed5f593a/Validez-de-contenido-y-juicio-de-expertos-Una-aproximacion-a-su-utilizacion.pdf
Evans, J. D. (1996). Straightforward statistics for the
behavioral sciences. Brooks/Cole Publishing
Facultad de Psicología de la Universidad
de Buenos Aires (2020). Recomendaciones psicológicas para afrontar la
pandemia. Autor.
http://www.psi.uba.ar/institucional/agenda/covid_19/recomendaciones_psicologicas.pdf
Fox, J., &
Bouchet-Valat, M. (2019). Rcmdr: R
Commander. R package version 2.5-2.
https://cran.r-project.org/web/packages/Rcmdr/index.html
George, D., &
Mallery, P. (2003). SPSS for Windows step
by step: A simple guide and reference. 11.0 update (4th ed.). Allyn &
Bacon.
Gorman, J. M. (1996).
Comorbid depression and anxiety spectrum disorders. Depression and anxiety, 4(4), 160-168.
https://doi.org/10.1002/(SICI)1520-6394(1996)4:4%3C160::AID-DA2%3E3.0.CO;2-J
Hogan, T. (2004). Pruebas Psicológicas. El Manual Moderno. Mc Graw Hill
Hyrkäs, K.,
Appelqvist-Schmidlechner, K., y Oksa, L. (2003). Validating an instrument for clinical
supervision using an expert panel [Validación de un instrumento para la
supervisión clínica mediante un panel de expertos]. International Journal of
nursing studies, 40(6), 619-625.
Kline, R. B. (2011). Principles and practice of structural
equation modeling. Guilford Press.
Lépine, J. P. (2002). The
epidemiology of anxiety disorders: prevalence and societal costs. The Journal of clinical psychiatry, 63,
4.
Magán, I., Sanz, J.,
& García-Vera, M. P. (2008). Psychometric properties of a Spanish version
of the Beck Anxiety Inventory (BAI) in general population. The Spanish journal of psychology, 11(2), 626.
https://revistas.ucm.es/index.php/SJOP/article/download/SJOP0808220626A/28750/0
McDonald, R.P. (1999). Test theory: A unified treatment.
Erlbaum.
Mineka, S., Watson, D.,
& Clark, L. A. (1998). Comorbidity of anxiety and unipolar mood disorders. Annual review of psychology, 49(1),
377-412. https://doi.org/10.1146/annurev.psych.49.1.377
Mountjoy, C. Q., &
Roth, M. (1982). Studies in the relationship between depressive disorders and
anxiety states: Part 2. Clinical items. Journal
of affective disorders, 4(2), 149-161.
https://doi.org/10.1016/0165-0327(82)90044-1
Muñiz, J. (2005). Análisis de los ítems. Editorial la Muralla.
Muñiz, J., Elosua, P., y Hambleton, R. K. (2013). Directrices
para la traducción y adaptación de los tests: segunda edición. Psicothema, 25(2),
151-157. https://www.unioviedo.net/reunido/index.php/PST/article/view/9910.
Nunnally, J. C., &
Bernstein, I. H. (1994). Psychometric
theory (3rd ed.). McGraw Hill.
Osman, A., Barrios, F.
X., Aukes, D., Osman, J. R., & Markway, K. (1993). The Beck Anxiety
Inventory: Psychometric properties in a community population. Journal of Psychopathology and Behavioral Assessment,
15(4), 287-297. https://doi.org/10.1007/BF00965034
Osman, A., Kopper, B. A.,
Barrios, F. X., Osman, J. R., & Wade, T. (1997). The Beck Anxiety
Inventory: Reexamination of factor structure and psychometric properties. Journal of clinical psychology, 53(1),
7-14.
https://doi.org/10.1002/(SICI)1097-4679(199701)53:1%3C7::AID-JCLP2%3E3.0.CO;2-S
Piotrowski, C. (2018).
The status of the Beck inventories (BDI, BAI) in psychology training and
practice: A major shift in clinical acceptance. Journal of Applied Biobehavioral Research, 23(3), e12112.
https://doi.org/10.1111/jabr.12112
Rajkumar, R. P. (2020).
COVID-19 and mental health: A review of the existing literature. Asian Journal of Psychiatry, 102066.
https://doi.org/10.1016/j.ajp.2020.102066
Revelle, W. (2018). Psych: Procedures for psychological,
psychometric, and personality research. R package version 1.8.12.
https://cran.r-project.org/web/packages/psych/index.html
Ritchie, H., & Roser,
M. (2018). Mental Health. Our World in
Data. https://ourworldindata.org/mental-health
Ruiz-Rodríguez, P. et al (2017). Impacto económico y carga de
los trastornos mentales comunes en España: una revisión sistemática y crítica.
Ansiedad y Estres, 23(2-3), 118-123.
https://doi.org/10.1016/j.anyes.2017.10.003
Sanz, J. (2014). Recomendaciones para la utilización de la
adaptación española del Inventario de Ansiedad de Beck (BAI) en la práctica
clínica. Clínica y Salud, 25(1),
39-48. http://scielo.isciii.es/pdf/clinsa/v25n1/original4.pdf
Sanz, J., & Navarro, M. E. (2003). Propiedades
psicométricas de una versión española del inventario de ansiedad de beck (BAI)
en estudiantes universitarios [The psychometric properties of a spanish version
of the Beck Anxiety Inventory (BAI) in a university students sample]. Ansiedad y Estrés, 9(1), 59–84.
Schumacker, R., &
Lomax, R. (2016). A beginner´s guide to
structural equation modeling. Routledge.
Stagnaro, J. C. et al (2017). Estudio epidemiológico de salud
mental en población general de la República Argentina. Vertex, 275. http://www.editorialpolemos.com.ar/docs/vertex/vertex142.pdf#page=36
Tinsley, H. E., y Weiss, D. J. (1975). Interrater reliability
and agreement of subjective judgments [Fiabilidad entre evaluadores y acuerdo
de juicios subjetivos]. Journal of Counseling Psychology, 22(4), 358.
Tornimbeni, S., Pérez,
E., Olaz, F., de Kohan, N. C., Fernández, A., y Cupani, M. (2008). Introducción a la psicometría. Paidós.