http://dx.doi.org/10.24016/2020.v6n2.157
ORIGINAL ARTICLE
Meanings Attributed by a
Group of Adult Men to the Experience of Having Type 2 Diabetes Mellitus
Significados atribuidos por
un grupo de hombres adultos a la experiencia de tener diabetes mellitus tipo 2
Gabriela
Vanegas 1, Alejandro Barbosa 1 * and Angie Zamora 1
1 Faculty
of Psychology, Universidad Antonio Nariño, Colombia.
*Correspondence: abarbosagonzalez@gmail.com
Received: January 23, 2020 | Reviewed: March 01, 2020 | Accepted:
April 20, 2020 | Published Online: May 01, 2020.
CITE IT AS:
Vanegas, G., Barbosa,
A., & Zamora, A. (2020). Meanings attributed by a group of adult men to the
experience of having type 2 diabetes mellitus. Interacciones, 6(2),
e108. http://doi.org/10.24016/2020.v6n2.157
ABSTRACT
Background: Diabetes is a chronic disease that causes various limitations in the
personal, family and social life of the person suffering from it. Aim: It was intended to analyze the
meaning attributed by a group of adult men to the experience of having diabetes
mellitus type 2. The methodology was qualitative with narrative design. The
technique to collect information was a free interview. The group of
participants consisted of four adult male parents diagnosed with diabetes
mellitus type 2. Intentional sampling was used for the selection. The
interviews were recorded in audio and literally transcribed. An inductive
categorical analysis was performed by means of matrices. There, similarities
and differences between participants were identified. Results: Among the findings it is highlighted that the impact of
the disease is presented in the personal, couple, family and work environment.
The main physical consequences are problems of vision, mobility and
insensitivity in lower limbs. On a psychological level feeling of sadness. Conclusion: The family plays a
fundamental role in dealing with the disease, since it constitutes a source of
support in adherence to treatment. It was evident in the children of the
participants a construction of meanings around the disease that minimizes its
impact. The above has the potential risk for risk behaviors to be repeated in
later generations.
Keywords: Meaning, Experience,
Diabetes Mellitus Type 2, Adult Men
RESUMEN
Introducción: La diabetes es una enfermedad crónica
que causa diversas limitaciones en la vida personal, familiar y social de la
persona que la padece. Objetivo: Se
pretendía analizar el significado atribuido por un grupo de hombres adultos a
la experiencia de tener diabetes mellitus tipo 2. Metodología: La metodología fue cualitativa con diseño narrativo.
La técnica para recolectar la información una entrevista libre. El grupo de
participantes estaba conformado por cuatro progenitores hombres adultos con
diagnóstico de diabetes mellitus tipo 2. Para la selección se utilizó un
muestreo intencional. Las entrevistas se grabaron en audio y se trascribieron
literalmente. Se realizó un análisis categorial inductivo por medio de
matrices. Allí se identificaron similitudes y diferencias entre participantes. Resultados: Dentro de los hallazgos se
resalta que el impacto de la enfermedad se presenta en lo personal, pareja,
familia y ámbito laboral. Las principales consecuencias físicas son problemas
de visión, movilidad e insensibilidad en miembros inferiores. A nivel
psicológico sentimientos de tristeza. Conclusiones:
La familia juega un papel fundamental a la hora de enfrentar la enfermedad, ya
que se constituye en fuente de apoyo en la adherencia al tratamiento. Se
evidenció en los hijos de los participantes una construcción de significados en
torno a la enfermedad que minimiza el impacto de la misma. Lo anterior tiene el
riesgo potencial para que se repitan comportamientos de riesgo en las
generaciones posteriores.
Palabras
clave:
Significado, experiencia, diabetes mellitus tipo 2, hombres adultos
BACKGROUND
Diabetes mellitus (DM) is considered a non-communicable chronic disease
that is related to high glucose levels due to the consumption of sugars and
proteins in excess and the consequent alteration of insulin production in the
pancreas. According to the Diabetes Atlas (International Diabetes Federation)
(IDF) (2019) report, globally there are 463 million people between the ages of
20 and 79 diagnosed with diabetes with a potential increase of 51% by the year
2045. In Central America and from the south, in the same age range, there are
32 million people with this diagnosis that tends to increase by 55% by the year
2045. The prevalence of the disease in this region and in this same age range
is 9.4 %, with Brazil, Paraguay and Chile being the countries with the highest
percentage of adults diagnosed with diabetes.
In Colombia it is estimated that 2 million people have been diagnosed; Sedó (2010) refers that older men are usually the ones who
report the greatest intensity of symptoms, since it generates feelings of
worthlessness, insecurity, social isolation and proximity to death. Due to the
above, they do not generate adherence to treatment behaviors (diet, physical
and pharmacological exercise). On the other hand, Pérez, Rivas and Martínez (2015) indicate that some adults do not have
problems with monitoring the treatment and management of diabetes, but if it
causes discomfort, not eating foods to their liking.
There is also the psychological impact. For González, Tinoco and Benhumea (2011), some
significant psychological responses are fear, anxiety, anger, depression, feelings of guilt and fear of abandonment by the
family. From this we can infer that family support for coping with diabetes is
essential. In this regard, Herrera, Quintero and Hernández (2007) argue that
the support network allows the person access to information and treatments. For
people with diabetes, family and social relationships can change since chronic diseases
have an impact not only on the people who suffer from them, but also on their
family and social network. These changes can be positive (union and support in
times of difficulty), but also negative (social isolation and
misunderstanding). Within the review of the state of the art made in this
research project, the few studies were observed from a qualitative perspective
with a narrative design that allows us to understand the experiences of people
diagnosed with diabetes. Therefore, the research objective was to analyze the
meaning attributed by a group of adult men to the experience of having type 2
diabetes mellitus to generate an approach to the experience of suffering from
this disease and offer reflections on their intervention.
Diabetes Mellitus Type
2
This type of diabetes is
characterized by high glucose levels and is defined by the World Health
Organization (WHO). (2018). as a chronic disease that occurs when the body does
not properly assimilate the insulin that is produced. Insulin is a hormone that
regulates the effect of sugar in the blood and that is why alterations in its
assimilation produce hyperglycemia that generates, in the long term, serious
health problems. For this reason, the diagnosed person must rigorously
follow medical treatment that focuses on managing insulin to achieve glycemic
control. According to Gil, Sil, Domínguez,
Torres and Medina (2013), it is important to explain to the person from the
moment of diagnosis that insulin is necessary depending on the evolution of the
disease. This is important, since therapeutic education is key to the proper
management of the disease.
Family and Illness
The contemporary family is the product of various historical and
cultural changes. Currently there are different types of family conformations.
As an example, we have the nuclear family, recomposed, single parent and single
parent among others. In each family there are particular characteristics
associated with the life cycle, communication, roles and hierarchy (Barbosa
& Jiménez, 2010). In general, the family is part of the support group that
people have and that usually goes through different stages in its process of
evolution and permanent change. All of the above implies adaptive challenges
for the group and each of its members.
One of the stressors that can affect family harmony is the appearance of
a chronic illness. Regarding the issue Rolland (2000) argues that the person
with a chronic disease is afraid that his life will end before his life
project, since the appearance of a disease interrupts the life project. n some cases the parents are taken
care of by their own children. Situation that can generate intergenerational
family conflicts (Ruiz, 2012; Placeres & León,
2011). Adult men, when perceiving the impact of the disease in their daily
life, give it a particular meaning (it varies from person to person) that is
born from a conglomeration of family interactions, socio-cultural beliefs and
individual particularities. According to Heredia and Pinto (2008).
METHOD
Type of Research and Design
The research is oriented from the qualitative approach. This is because
it is intended to track reality from the perspective of the participants. The
research interest is centered on meaning, narration, understanding and action (Rodríguez,
2011).
As for the design, it is narrative, which implies the use of data
collection techniques such as individual and group interviews. There people can
relate their experiences spontaneously. For Barbosa, Reyes and Escobar (2009),
from the moment that people narrate their life experiences, they update their
story and the experiences return as images. Fernández, Hernández and Baptista (2014), argue that narrative designs have
to do with the succession of events, phenomena and processes. Thoughts,
feelings and interactions are involved there. The above arises thanks to the
direct narration of the protagonists. Finally, Cardona and Alvarado (2015) add
that from this perspective reality is understood as a social construction. Due
to the above, the approach to the world is mediated by the subjects and their
experience.
Technique for Gathering
Information
The technique used was the unstructured interview, which seeks the
information that is needed through defined topics or focuses. Díaz, Torruco, Martinez and
Varela (2013) state that this type of interview is informal and flexible,
whereby it adapts to contextual conditions. However, this does not prevent us
from delving into the subject and detailing relevant aspects for the research.
Through the question and answer, the life reconstruction of the interviewed
person is achieved and in his story the meaning that the person has about an
experience or topic addressed is reflected, in this case the experience of
suffering from Type 2 Diabetes Mellitus.
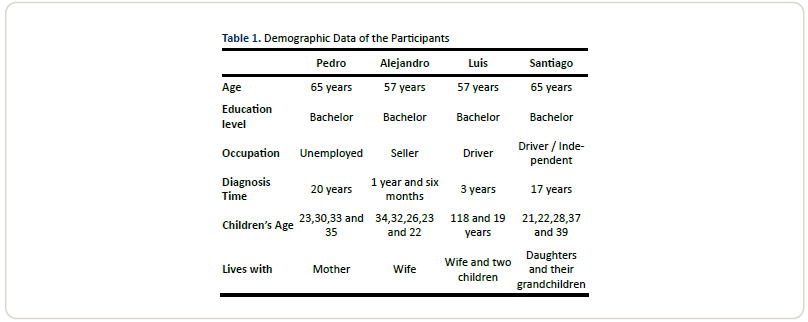
Participants
Four participants were selected for this research. The inclusion
criteria consisted of: being adult men (50-70 years of age), having a diagnosis
of type 2 diabetes mellitus, being parents and having at least secondary
education; This population was selected since, as reported by Sedó (2010), older adults may suffer the effects of
diabetes with greater intensity; Additionally, type 2 diabetes mellitus is more
recurrent in adults than in any other age group. (Palacios – Barahona, Arango-Posada, Ordoñez, Alvis-Guzmán. 2019).
The demographics of the participants are described below. The above
taking into account the principle of confidentiality.
Process
At the beginning, 12 potential participants belonging to a research
project of the Universidad Antonio Nariño in Bogotá on diabetes prevention were
located. After conducting an exploratory interview, the inclusion criteria were
established and the four were finally selected for open interviews. The
technique for selection was intentional sampling. Two meetings were held for
the interview. In the first, the objectives and justification of the study were
made explicit. After generating empathy and resolving concerns about
participation in the work, a second meeting was held to sign the informed
consent and interview. The interview was audio recorded for later literal
transcription and analysis. The analysis developed is of the inductive
categorical type. For this purpose, meaning matrices were used where the
fragments of the most recurrent interviews were organized within the stories of
the interviewees. With this material, the categories that allowed the analysis
to be carried out were inferred. These categories were: Meanings attributed to
the diagnosis and acceptance of the disease, meanings attributed to the
psychological consequences and adherence to treatment; meanings attributed to
changes in relationships with children and partner. Finally, meanings
attributed to limitations in sexual and work life.
RESULTS AND DISCUSSION
Meanings Attributed to
the Diagnosis and Acceptance of the Disease
This category refers to the medical and environmental history of the
disease. Also, to the physical impact generated by the disease. From this, the
experiences associated with the symptoms and the limitations that this disease
generates in people appear.
Most of the participants mentioned a history of diabetes in their family
history. However, they do not associate this fact with the development of this
disease in their personal history. Luis's story (3 years diagnosed): My
brothers told me that my grandmother died of diabetes. Santiago (17 years
diagnosed): My dad died of diabetes and so did my brother. When I found out
that they had this disease, I continued everything calm. One in good health does
not think that one can get sick with diabetes.
Regarding environmental antecedents, the participants recognized eating
habits that are characterized by unhealthy food intake. Alejandro (1 year and
six months diagnosed): I think I got sick from eating junk food on the street.
Fried and sodas. Santiago (17-year-old diagnosed): I practically ate at odd
hours, but now I can't eat at set times either. Likewise, family biological
antecedents, as well as eating habits are recognized as determining elements in
the onset of the disease. According to Colombie, Socca, Rivas and Borrego (2016): “Family history of
diabetes, hypertension (HT), obesity and environmental factors play an
important role in the emergence and development of the disease” (p. 125). For
participants, the first symptoms of the disease are the ones that raise the
alarm about the situation, but it is as a result of the diagnosis that one
becomes aware that diabetes is a disease that puts health at risk. Pedro (20
years diagnosed): I was working in Yopal, that day we
went to eat a bite, everything was fine, but then I felt bad. I was very
thirsty for 20 days. I couldn't go to the bathroom and I didn't feel like
eating. I thought lunch was spoiled. Alejandro (1 year and six months
diagnosed): Diabetes is totally silent; this disease does not manifest itself
with anything. One day he wakes up. You feel dizzy, you've never felt that
dizziness. I felt totally dizzy and also very thirsty, I didn't know why, so
they went to hospitalize me. Regarding the topic Sedó
(2010) explains that diabetes is usually asymptomatic. You can have high blood
glucose levels without presenting symptoms. The reports of the participants
show the general ignorance of DM2 in terms of characteristics, predisposing
factors and consequences. The consequence of this is that they do not act
preventively despite the history of the disease in the family. In the same way,
the diagnosis of the disease takes them by surprise. Alejandro (1 year and 6
months diagnosed): It was surprising, me and my wife
were surprised. They had told her when I had cancer that I was pre-diabetic and
well, she took good care of herself for two or three months, but she was cured.
And when they tell me that I already have diabetes, we didn't know what to do.
Luis (3 years diagnosed): When I found out I was very scared, I told my wife,
she was also very scared, and we were not aware of the disease. Regarding the
limitations generated by the disease, the participants recognize and accept
them; These limitations are associated with mobility
problems, decreased vision and numbness in the lower limbs. Luis (3 years
diagnosed): Previously I ran and had strength, now not. I have felt
deterioration in my vision and at times I get the diabetic foot. Pedro
(20-year-old diagnosed): Now I can't walk a lot or stay standing. Sometimes I
am walking and suddenly I fall with my cane. Also, I have had various skin
complications because I don't have that sensitivity from before. Sometimes I
can't feel my feet.
Meanings Attributed to
Psychological Consequences and Adherence to Treatment
In this category appear experiences related to psychological discomfort
and also the difficulties of the participants to achieve adherence to the
treatment adequately. Family support and religious beliefs are also
highlighted.
The psychological consequences are associated with a greater recurrence
of feelings of sadness and loneliness: Alejandro (1 year and 6 months
diagnosed): The psychological ones, thinking about what is happening in my life
and being afraid of dying. Santiago (17 years diagnosed): Yes, it makes me very
sad, I feel down, but I try to control myself. According to different authors
(Rolland, 2000; Jiménez & Dávila, 2007),
psychological reactions of sadness, fear of death, loneliness and even
depression are usually common in individuals with chronic diseases; To this it
can be added that the treatment of diabetes requires a significant change in
life behaviors, which causes emotional reactions of anguish and frustration.
(Canales & Barras. 2014).
The main source of information on DM2 are dietitian doctors, who provide
essential guidelines to obtain greater adherence to treatment. Participants
mention following medical recommendations such as taking and applying
medications, nutritional care and physical activity. Paradoxically, they show
difficulties in following the same indications. This is due to the fact that
some people self-medicate or handle negative beliefs regarding the medications
prescribed by the doctor. Pedro (20 years diagnosed): I get up and make
breakfast, then half-nines, lunch, I take ounces, around 10:00 am I take
insulin, I apply 10 cm of insulin to my stomach and a lot of nutritional care.
Luis (3 years diagnosed): Well the doctors told me to take care of my food.
From there I have come judicious. That's why I have a coffee with whole wheat
bread, but sometimes I think that I would rather die full than hungry. Santiago
(17 years diagnosed): I did not want insulin and it lasted for three months, I
administered insulin and mixed herbs. I stopped it myself, but I kept taking
four pills. In relation to compliance and difficulties with adherence to
treatment in parents, Alves, Castro, Ribeiro and
Faustino (2007) state that for there to be a favorable evolution in the
treatment of diabetes, there must be self-regulation of behavior.
Hoyos, Arteaga & Muñoz
(2011), identify, in their research on factors that limit treatment in diabetic
patients, emotional, food and religious perceptions as a turning point in the
treatment of diabetics; At the same time, they propose
the understanding of sociocultural beliefs as part of the interventional
process to increase the effectiveness of the treatment. However, despite all of
the above, the study participants are motivated to continue fighting the
disease. What is
described below has more to do with their family than with their life projects
or themselves.. Luis (3 years diagnosed): I take my medications for my children and my
wife, my family. I want to be okay for them.
Meanings Attributed to
Changes in Relationships with Children and Partner
In this case, experiences associated with changes in family interactions
that have to do with the appearance of the disease are evidenced. Among these
changes is the supportive reaction of the children of the participants.
Likewise, the role of the couple is observed regarding adherence to treatment
and when assuming hierarchical responsibilities.
In the participants' narratives the theme of the individuation of
children and the formation of new homes predominates. Which has repercussions
in the construction of a new family dynamic, Pedro (20 years diagnosed): I am
not saying that my children do not collaborate with me, but if I feel as if I
am asking for alms and the times I have gotten sick, I tell my daughter. She is
by my side. My children have to answer for their home, she wants to be with me,
but she can't. Luis (3 years diagnosed): Since the disease we continue to share
the same, we do not share the same food, but the other things do. My children
call and are waiting on me. Although they already have their homes. Santiago
(17 years diagnosed): I have been far away from my younger daughters; they are
already making their lives. The children of the participants withdraw due to
their responsibilities and this withdrawal possibly leads to misinformation
about a disease that is potentially heritable. Alejandro (1 year and 6 months
diagnosed): I feel that for them everything related to the disease is normal,
perhaps because they think that cancer was harder than diabetes, and since I
came out of cancer, they believe that I can get out of this disease
, I don't need your support. A construction of meanings around the
disease that minimizes its impact is evidenced in the children of the
participants. This can influence the repetition of risk behaviors in later
generations. In this case, the disease can be inherited as well as the beliefs
and behaviors associated with the problem. For Rolland (2000) the asymptomatic
of a chronic disease reinforces confusion and disorientation in various ways.
This makes denial easier for people with the disease and their families to use.
The result is the minimization of the effects of the disease.
The partner of the participants is also an important source of support
for treatment management. Alejandro (1 year and 6 months diagnosed): He has
changed a lot; he is out of the ordinary. Life as a couple changed. Now we talk
a lot about our diseases and therefore also about the company, but more about
the disease. She has always been with me and more in my illnesses. Luis (3
years diagnosed): At the beginning of the disease, everything began to change.
I have tried to control my illness to share with her. I have learned to live
with the disease, I think we all do that and more because she is who is with
me. Sometimes she has to be responsible for imposing rules and assuming certain
responsibilities that previously corresponded to me. Due to the limitations
generated by the disease, changes appear regarding the distribution of
responsibilities and management of authority. In most cases, it is the partner
of the participants who assumes responsibilities and authority to equalize the
family hierarchy. According to Mendizábal and Pinto
(2006), it is important that within family interactions there is a clear
hierarchy. This regardless of the vital moment and the situation faced. All of
the above is related to what was expressed by Hernández (1997), who points out
that the true family challenge lies in facing non-normative stressors, such as
chronic disease, reorganizing itself as a form of family resource that
ultimately allows the family to adapt to new situations.
Attributed meanings to limitations in sexual and work life
In this category, the most significant limitations that the participants
express in the experience of having DM2 are condensed. Particularly in sex and
work life. Experiences associated with physical and psychological difficulties
are highlighted
Sex life in the couple decreases significantly. This is linked to the
physical consequences of the disease. There are observed alterations in the
control of the body and psychological consequences such as depression that
reduces the desire for the other person. Pedro (20 years diagnosed): You lose
everything, for example, you don't feel like being with her anymore. That is
instantaneous and the battery does not work. The first thing they think is that
you have another person. Luis (3 years diagnosed): There are times when
everything changes with the couple. Before I was normal with my partner. Before
we had relationships three times a month and now once and that. Alejandro (1
year and 6 months): Life as a couple is out of the ordinary, it is a very
drastic change. There is no more of that between us. For Lendon
and Castelo (2013),
There is also evidence of deterioration in the workplace, since
performance is not the same. The above due to physical limitations and the
feeling of social isolation. Alejandro (1 year and 6 months): As long as I
work, I can continue with my normal life. Commerce requires me to continue and
every day it asks me for more products. This expands my micro business and
makes me more profitable. But I also have to ask someone to help me at work.
It's a limitation, I can't push myself. Luis: Diabetes makes you sleepy, I try
to sleep at times. Santiago (17 years diagnosed): At the beginning, yes, I had
a little more than two years that I could not work. There everything decayed,
automatically I stayed at zero. But I continued.
CONCLUSION
A lack of knowledge of diabetes and a lack of recognition of the risk
factors that make its development possible are observed within the
participants' reports. This despite having a family history of diabetes. As the
main physical consequences, the participants identified problems with vision,
mobility and insensitivity in the lower limbs. On a psychological level feeling
of sadness and fear towards the development of the disease.
On the other hand, the family plays a fundamental role when facing the
disease, since it constitutes a source of support for adherence to treatment.
The partner of the participants happens to have the greatest hierarchical and
sometimes economic burden. A construction of meanings around the disease that
minimizes its impact is evidenced in the children of the participants. This has
the potential risk for risk behaviors to recur in subsequent generations.
In addition, the sexual life in the couple decreases significantly. This
is linked to the physical consequences of the disease. There are observed
alterations in the control of the body and psychological consequences such as
depression that reduces the desire for the other person. There is also evidence
of deterioration in the workplace, since performance is not the same. The above
due to physical limitations and the feeling of social isolation.
Regarding the limitations of the study, the time established for the
development of the project did not allow locating more participants. Likewise,
there were no female participants to be able to contrast possible differences
and similarities by gender and role within family relationships.
ORCID
Gabriela
Vanegas https://orcid.org/0000-0003-1462-7720
Alejandro
Barbosa http://orcid.org/0000-0003-1400-2042
Angie Zamora https://orcid.org/0000-0002-9629-2591
FUNDING
This study was self-funded.
CONFLICT OF INTERESTS
The authors
state that there were no conflicts of interest when writing the manuscript.
REFERENCES
Alves,
J., Castro, C., Ribeiro, H. & Faustino, H. (2007). La incertidumbre en la
enfermedad y la motivación para el tratamiento en diabéticos tipo 2. Revista Latino Enfermagem,
15(4), 1-10. Recuperado de http://www.scielo.br/pdf/rlae/v15n4/es_v15n4a09.pdf
Atlas
de Diabetes (International Diabetes Federation) (IDF)
(2019). IDF Diabetes atlas. Novena edición.
Barbosa,
A. & Jiménez P. (2010). Significados asignados al establecimiento de
vínculos afectivos y la posible conformación familiar por parte de jóvenes
adultos homosexuales. Revista Vanguardia
Psicológica, 1(1), 33-51.
Barbosa,
A., Reyes, S. & Escobar, M. (2009). Narrativas dominantes de personas
privadas de la libertad en torno al concepto de familia. Umbral Científico, (14), 170-180.
Canales
& Barra, E. (2014). Autoeficacia, apoyo social y adherencia al tratamiento
en adultos con diabetes mellitus tipo II. Psicología y salud. Vol 24 Num. 2: 167-173. Recuperado de: http://psicologiaysalud.uv.mx/index.php/psicysalud/article/view/922
Cardona,
A. & Alvarado, S. (2015). Investigación narrativa: apuesta metodológica
para la construcción social de conocimientos científicos. Revista Ces psicología, 8(2), 171-181. Recuperado de http://revistas.ces.edu.co/index.php/psicologia/article/view/3022/2427
Columbíe, Y., Soca, P.,
Rivas, D. & Borrego, V. (2016). Factores de riesgo asociados con la
aparición de diabetes mellitus tipo 2 en personas adultas. Revista Cubana de endocrinología 27(2), 123-133. Recuperado de http://scielo.sld.cu/pdf/end/v27n2/end02216.pdf
Díaz,
L., Torruco, U., Martinez,
M. & Varela, M. (2013). La entrevista, recurso flexible y dinámico. Revista investigación en Educación Médica,
2(7), 162-167. Recuperado de https://www.redalyc.org/pdf/3497/349733228009.pdf
Fernández, R. Hernández, C. & Baptista, M. (2014). Metodología De La Investigación. Recuperado
de http://observatorio.epacartagena.gov.co/wp-content/uploads/2017/08/metodologia-de-la-investigacion-sexta-edicion.compressed.pdf
Gil,
L., Sil, M., Domínguez, E., Torres, P. & Medina, J. (2013). Guía de
práctica clínica diagnóstico y tratamiento de la diabetes mellitus tipo 2. Revista Med inst seguro soc, 51(1) 104-119. Recuperado
de https://www.medigraphic.com/pdfs/imss/im-2013/im131o.pdf
González,
N., Tinoco, A. & Benhumea, L. (2011). Salud
mental y emociones en pacientes con enfermedades crónico- degenerativas. Un
acercamiento a la diabetes mellitus tipo 2. Revista
Espacios públicos, 14(2), 258-279. Recuperado
de http://www.redalyc.org/pdf/676/67621319013.pdf
Heredia,
J. & Pintó, B. (2008). Depresión en diabéticos: un enfoque sistémico. Revista Ajayu,
6(1), 22-41. Recuperado de http://www.scielo.org.bo/pdf/rap/v6n1/v6n1a2.pdf
Hernández,
A. (2009). Familia, ciclo vital y
psicoterapia sistémica breve. Bogotá: Búho.
Herrera, L., Quintero, O. &
Hernández, (2007). Funcionalidad y red de apoyo familiar en pacientes
diabéticos tipo 2 servicio de endocrinología Iahula
Mérida. Revista Academia, 6(12), 62-72.
Recuperado de http://www.saber.ula.ve/bitstream/handle/123456789/27301/articulo6.pdf;jsessionid=04E4AD2DE1024D0956270EA7BCDAA4BF?sequence=1
Hoyos,
T., Arteaga, M &Muñoz, M. Factores de no adherencia al tratamiento en
personas con diabetes Mellitus tipo 2 en el domicilio. La visión de un
cuidador. Invec. Educ. Enferm. 29(2): 194-203. Recuperado de: http://www.scielo.org.co/scielo.php?script=sci_abstract&pid=S0120-53072011000200004
Jiménez,
C. & Dávila, M. (2007). Psicodiabetes. Revista Avances en psicología
Latinoamericana, 25(1), 126-143. Recuperado de http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S1794-47242007000100012
Lendon, L. & Castelo, E. (2013).
Afrontamiento al distres relacionado con la
disfunción eréctil en varones con diabetes mellitus tipo 2. Revista Cubana endocrinología, 24 (3), 242
-257. Revisado de http://scielo.sld.cu/pdf/end/v24n3/end02313.pdf
Mendizabal, O. & Pinto,
B. (2006). Estructura y diabetes. Revista
Ajayu, 4(2), 191-211. Recuperado de http://www.scielo.org.bo/pdf/rap/v4n2/v4n2a3.pdf
Organización Mundial de la Salud (OMS).
(2018). Recuperado de: https://www.who.int/es/news-room/fact-sheets/detail/diabetes
Palacios-Barahona,
U., Arango-Posada, M., Ordoñez, JE & Alvis-Guzman,
N. (2019). Calidad de vida de pacientes con diabetes tipo 2 en Colombia.
Revisión sistemática y metaanálisis acumulativo. Rev. CES Psico. 12(3),
80-90. Recuperado de: http://www.scielo.org.co/pdf/cesp/v12n3/2011-3080-cesp-12-03-80.pdf
Pérez,
Z., Rivas, V. & Martínez, A. (2015). Percepción del apoyo familiar y
dificultades relacionadas con la diabetes en el adulto mayor. Revista Horizonte sanitario, 14(1), 14-20. Recuperado
de https://biblat.unam.mx/es/revista/horizonte-sanitario/articulo/percepcion-del-apoyo-familiar-y-dificultades-relacionadas-con-la-diabetes-en-el-adulto-mayor
Placeres,
J. & León, L. (2011). La familia y el adulto mayor. Revista Med. Electrón, 33(4), 472 – 483. Recuperado
de http://scielo.sld.cu/pdf/rme/v33n4/spu10411.pdf
Rodríguez,
J. (2011). Métodos de investigación cualitativa. Revista de la corporación Internacional para el Desarrollo Educativo,
(8), 1-34. Recuperado de http://www.cide.edu.co/doc/investigacion/3.%20metodos%20de%20investigacion.pdf
Rolland, J. (2000). Familias,
enfermedad y discapacidad. Una propuesta de la terapia sistémica. España,
Barcelona. Gedisa.
Ruiz, J. (2012). Aspectos
biopsicosociales que incides en la salud del adulto. Revista Cubana de medicina general integral, 28(2), 79-86. Recuperado
de http://scielo.sld.cu/pdf/mgi/v28n2/mgi09212.pdf
Sedó,
P. (2010). Percepciones sobre la diabetes y su padecimiento en personas adultas
mayores diabéticas y familiares en un área urbana de Costa Rica. Revista Anales en Gerontología, 6(6),
99-112. Recuperado de https://dialnet.unirioja.es/servlet/articulo?codigo=6140284